






2017.09.08 第19回 An Interview with Dr. Robert M. Ricketts 1987
2017.08.17 第18回 An Interview with Dr. Robert M. Ricketts 1987
2017.08.08 第17回 An Interview with Dr. Robert M. Ricketts 1987
2017.08.01 第16回 An Interview with Dr. Robert M. Ricketts 1987
2017.07.26 第15回 An Interview with Dr. Robert M. Ricketts 1987
2017.07.24 第14回 An Interview with Dr. Robert M. Ricketts 1987
2017.07.20 第13回 An Interview with Dr. Robert M. Ricketts 1987
2017.07.03 第12回 An Interview with Dr. Robert M. Ricketts 1987
2017.04.25 第11回 An Interview with Dr. Robert M. Ricketts 1987
2017.03.17 第10回 An Interview with Dr. Robert M. Ricketts 1987
2017.01.18 第9回 An Interview with Dr. Robert M. Ricketts 1987
2016.08.27 第8回 An Interview with Dr. Robert M. Ricketts 1987
2016.08.24 第7回 An Interview with Dr. Robert M. Ricketts 1987
2016.08.19 第6回 An Interview with Dr. Robert M. Ricketts 1987
2016.08.05 第5回 An Interview with Dr. Robert M. Ricketts 1987
2016.07.06 第4回 An Interview with Dr. Robert M. Ricketts 1987
2016.06.17 第3回 An Interview with Dr. Robert M. Ricketts 1987
2016.06.11 第2回 An Interview with Dr. Robert M. Ricketts 1987
2016.06.07 第1回 An Interview with Dr. Robert M. Ricketts 1987
2016.03.23 「サイエンス」って?
2016.03.01 うぐいすの みをさかさまに 初音かな
第19回 An Interview with Dr. Robert M. Ricketts 1987
2017.09.07
第19回:Muscular Environment “筋肉”という環境
An Interview with Dr. Robert M. Ricketts DDS, MS April 13, 1987
Copyright © 2015 University of Michigan School of Dentistry
Some rights reserved. Except where otherwise noted, this work is licensed under the following:
Attribution: Please attribute the work to the University of Michigan School of Dentistry and any individual author(s) cited. Not-for-profit: Use, display, and redistribute all or part of this work for non-profit and educational purposes only.
Share alike: Redistribute derivative works with the license listed here.
Visit the University of Michigan School of Dentistry’s website at http://www.dent.umich.edu/.
View the original interview at https://www.youtube.com/watch?v=lcBLmVOn3m0.
Interview conducted by James McNamara, DDS, MS, PhD. Interview transcribed by Yuri Shindo, MD.
Interview translated by Katsuyuki Shindo, DDS, PhD.
【 Muscular environment 】
〔M.〕 Now you mentioned the lower labial region. Something that’s of particular concern to me and my family is this question of — what do you call it - a“sub-labial release”.
【 “筋肉”という環境 】
〔M.〕 次にお尋ねしたいのが、下唇の領域に関する内容です。私自身、そして家族の者にも関係している事柄なのですが…正式には何と呼ぶのか分かりません。サブレイビアルリリース(下唇溝の過剰緊張を解放する処置)と呼んでよろしいでしょうか?
〔R.〕 Sub-labial release. Yes.
〔R.〕 そのような呼び方でもよろしいでしょう。
〔M.〕 Do you want to describe that a bit? And how that fits into what we’re talking about.
〔M.〕 今話していることに関連させて解説を頂けますか?
〔R.〕 Well, I suppose my respect for the lower lip started with a patient that McGonagle, in my class, treated. As you know, we had McGonagle and Kincaid from Ohio; Elbert King from Illinois; Samuel Pruzansky from Baltimore — er, New York; myself from Indiana; Walter from over here at Niles, Michigan; Edmund Wong from Hawaii; and Guy Wood who went to Portland. And that constituted our class at that time.
I had, in January [of 1948] of our class, we took impressions on the waiting list. And we took them all in plaster, incidentally. Did you know that?
〔R.〕 下唇の筋肉に大きな興味を抱いたのは、同僚のマッガンゴル氏が担当した 14歳の少女の治療の時です。同級生のことをふと思い出したので、あなたもご存じかと思いますが、少し紹介しておきましょう。マッガンゴル氏の他に、オハイオ州出身の Dr. Robert Kincaid、イリノイ出身の Dr. Elbert King、メリーランド州ボルティモア出身の Dr. Samuel Pruzansky、インディアナ州出身の私、この近くのミシガン州のナイルズ出身の Dr. Douglas Walter、ハワイから来た Dr. Edmund Wong、オレゴン州のポートランドに行った Dr. Guy Wood らがいました。このメンバーによって当時のクラスは編成されていました。
1948 年 1 月、歯列の印象採得の困難な、下唇がひどく引き締まっている患者が治療待ちリストに居ました。ついでながらお話しすると、当時は石膏を用いた印象採得法が一般的であり、私たちはすべての患者の歯列を石膏で型取っていました。ご存じでしたか?
〔M.〕 I would imagine that that might be the case.
〔M.〕 なんとなく想像がつきますね。
〔R.〕 That was the discipline. And we trimmed our models by hand. We weren’t permitted to use a model trimmer. Did you know that?
〔R.〕 訓練の一環です。石膏模型トリーマーの使用を禁止されており、模型のトリミングは手作業で行っていました。
〔M.〕 No, I didn’t know that. Jeez!
〔M.〕 すさまじい教育だったのですね!
〔R.〕 Can you imagine cutting those with a jack plane, and filing them and polishing them? Your hands were re-bleeding. You wanted discipline? That was discipline.
Well anyway, I took impressions of this patient. Her name was Erica Rafting. She had the most vicious lower lip habit that I had ever seen. Brodie had never seen anything like it. I happened to take her on the waiting list. And I noticed how tough that lip was when getting an impression of the kid’s mouth.
Anyway McGonagle came up to a case that Brodie had selected for his day. And he elected to put a shield on that case, to strap up the lower arch as Brodie liked to do. And he built a shield off of an .022 × .028 wire double back soldered, and this shield was out there to hold the lower lip away, to lock these incisors. Now if you can imagine a case with eight front teeth all in a line. That’s just about the way it was! All crumpled up and all in one straight line here. So I was there watching the day that McGonagle put it in. And he put it out there maybe four millimeters or five millimeters, maybe that much ahead of the lower arch. That patient came back in two weeks and that appliance was completely buried in her lip. It was up and under this way, and over the top this way. It was buried. That lip was so tight that it just wrapped all the way around that thing. She was bleeding all over the place.
They stayed with it. They backed it up a little bit. It was kind of experimental because I don’t think Brodie had ever used it before. He called it a“shield.”And I followed that case, even after McGonagle had left. Well can you imagine that that lower lip was so strong that he treated that case with Class II inter-maxillary elastics, and got all of the [upper] teeth in the lower arch, and the lower molar ended up posterior to where it started, all due to the contraction of that lower lip? So that experience I had before I went to California.
Then, I went to California - of course I was on headgears - and I entertained the idea of making [the appliance] simpler, putting buccal tubes on the lower molars, and putting in what I called the“bumper” to push the lower teeth and lower lip out so that we could let the lower teeth have space. Well, I began to use that quite a bit, and I found that within two weeks, sometimes you got a change in the oral environment that was quite favorable. It was amazing because you wouldn’t notice that the child even had it in two or three weeks.
Well anyway, on those severe cases when I put it all the way down in the sulcus here, not on this part of the lip - this is loose and flaccid. It’s not going to have much resistance. But if you get it down into this level right here, that is extremely tight, and we found that we were actually moving molars bodily distally with this bumper, and of course impacting the back teeth.
So that gave me respect, then, if that could do that with a bumper, then the whole lip intact holding the occlusal plane down, that’s a part of our whole anchorage belief, as you understand. And that became the problem.
Now, what to do in those patients in which you deliberately wanted to displace the lower arch forward? You didn’t want to treat to the environment. How are we going to handle that?
Well, for several years, I went into lip-blowing exercises, trying to stretch it, pursing the upper [lip], blowing it. I got that technique from a guy from Scotland, who came through Illinois one time. And so that’s what we tried to do. This was long, hard, and you wouldn’t get cooperation from the patient.
So about ten years ago or so, we entertained the idea of surgically relieving the lower lip. I’d worked with Warren Hamula ten years before that when he, together with the surgeons and periodontists at Colorado Springs, Colorado, had done some experimental work. And they had sort of given it up because they didn’t quite feel that it was enough difference to make a difference. But they were only working down in here. They weren’t working up in here. They were working down in here relieving the mentalis. They felt that it was just the mentalis, mentalis, mentalis. Well, no, that’s not what it is because this is not the mentalis up here. The mentalis start here and goes down. This crease is right here. So I said“, Well that has to be then either the orbicularis oris, the incisivus inferioris - that’s a horizontal muscle going across - or the quadratus labii.”And according to Cunningham, almost a quarter of the population has a union of the quadratus in the midline across the chin. These buttons on the chins that you see.
Remembering that, I said, “Well, maybe the problem is one of transecting that muscle mass that’s going from side to side,” because this was all hypertrophied. You pick that up in a patient here with Class Ⅱ Division 2, or even 1, in which they’ve done this muscle has... it’s like weightlifters. And it’s even gone to the place where it’s advanced now maybe to fibrous connective tissue.
So we had a patient on a surgical table that was getting a genioplasty done. And I’d been talking to the plastic surgeon about this for a long time, Henry Kawamoto, who I worked with a great deal. And he said, “Wait a minute. What is that you’ve been talking about?” We had this patient with the lip all laid open, and he pulled it upside down and looked at it. I said, “That’s it! Right there.” So he said, “You want to do this?” We cut, cut. And I said“, You want to take that out?”So he stripped it out. That’s what I want to do. So the first one we did was on a patient that had an advancing genioplasty with this tight lip. Even with an advancing genioplasty, you’re going to end up with some of these creases in here that really are tough. And so this needs to be done even though you’re doing a chin procedure. So with that then, I started experimenting with patients and to date I’ve done ninety of them.
〔R.〕 石膏模型を粗かんなで下削りし、やすりをかけて磨いていたので手を切って出血することもしばしば…、あなたもやってみたいですか? とにかく体に覚えこませる訓練でした。
ともあれ、このエリカ・ラフティンという少女の歯列印象を私が採りました。驚くほど強力な下唇の習癖があり、彼女ほどの症例はブローディ教授もお目にかかったことがなかったくらい…。治療待ちリストから彼女を選んだのも偶然のことでした。子どものわりには極めて強靭な下唇の筋肉… 印象を採るときに気づきました。
ともあれ、その日当番にあたっていたマッガンゴル氏が、ブローディ教授の指示で治療を担当することになりました。ブローディ教授の好む治療法として、まず下顎歯列全体にブラケットをつけ、ワイヤーの前方部にシールドを設けました。シールド用の 0.022×0.028 ワイヤーが後方で折り返されて主線にろう着されたタイプです。これによって下顎切歯が下唇の圧迫から解放されることを期待しました。筋肉の張りの強さで、8 本の前歯が一直線に並んでいる姿がご想像できますでしょうか? まさしく、前歯がくしゃくしゃになったまま一直線に並んでいるのです。マッガンゴル氏が主線にろう着したシールドをその子に装着するのを横で眺めていました。たしか 4〜5mm ほど前歯から離していたと思いますが、もっと離れていたかもしれません。2 週間後、患者が来院したときには装置が口唇の内側に埋まり込んでいました。あまりにも口唇の緊張が強いので、下からも上からも、粘膜が装置を巻き込んでしまい、口中血だらけでした。
方法自体は変更せず、シールドを少し後方へ移動させました。たぶん実験的に行っていたのでしょう、というのも、ブローディ教授にはどうやらこの方法を採用したことのある節がなかったからです。彼はこの装置を「シールド」と呼んでいました。マッガンゴル氏が大学を去った後も、私はこの患者の観察を続けました。Ⅱ級顎間ゴムを用いて上顎歯列を下顎歯列の位置まで後退させたのにもかかわらず、下顎大臼歯がなんと治療前よりも後ろの位置に移動していたわけですから、これほど強力な下唇は滅多にはお目にかかれないでしょう。 全てが下唇の拘縮に起因していたように思われました。カリフォルニアで開業する前の経験です。
その後、カリフォルニアに渡ってヘッドギヤーを使った治療を行う一方、術式を単純化しようと装置の改良を重ねていきました。下顎大臼歯の頬側チューブにバンパーと呼ばれる装置を取り付け、下唇の圧力を歯列から排除して下顎の歯列にスぺースが生まれるような工夫をしました。かなり多くの症例にバンパーを用いた結果、2 週間以内に口腔内の環境が改善されるのを発見しました。子どもたちが僅か 2〜3 週間、この装置を使っただけとは思えないほどの変化でした。
重篤な症例においてはバンパーを下唇に当てるのではなく、下唇溝の場所まで降ろした方が効果は上がります。上の位置では組織が柔らかいので十分な抵抗が得られません。しかし、この下唇溝のレべルまで下げると、そこにはきわめて引き締まった組織が存在します。その部分にバンパーが触れるようにすれば、下顎の大臼歯が遠心へ歯体移動するほどの効果が発揮されます。勿論、後方歯を埋伏させるほどの力です。
ですから、私は大いに注目したのです。バンパーを用いればこのような歯の移動が可能となる事実や、あるいは口唇が元の状態を維持したまま、咬合平面も保たれるとなれば、それが新たなアンカレッジの概念にもなるわけです。ところが一端において、(この下唇溝の緊張が強すぎた場合) これは問題にもなります。
では、(後方に引っ込みすぎている)下顎歯列をあえて前に移動させようと試みる場合は、どのような処置を行うのが望ましいのでしょう? 従来の考えでは、口腔内環境の変更は不可能とされていたので、積極的に挑む人は少数でした。このような症例をどう扱えばよいのでしょうか?
口唇を伸展させるために、唇をすぼめる練習や上唇の内側に空気を溜めて膨らませる訓練に私は数年間かかずらってきました。この訓練は、イリノイ大学に一時期在籍していたスコットランド出身の臨床家に教わったものです。なんとかして口腔内環境を改善しようと私は努めていたのです。ところが彼の訓練法は、長期の忍耐を患者に要請するためなかなか協力を得られませんでした。
そのようなわけで、今から 10 年程前、あるいはもう少し遡りますが、外科処置によって下唇の締め付けを解放する試みを検討してみることにしました。コロラドスプリングスにおいて、外科医や歯周専門医と仕事をしていたワーレン・ハミュラー氏と、私はいくつかの実験的な研究を開始しました。当初はいくら術式を工夫してもあまり成果がみられないので彼らは半ば諦めている状態が続いていましたが、私から見ると、彼らの採用していた術式は、下方のこの部分に限られており、肝腎のこの領域には手をつけていませんでした。その方法ではオトガイ筋の力を緩衝させるだけに過ぎません。オトガイ筋のことばかりに意識が引きづられているきらいも感じられました。実は下唇の締め付けというものは、下方に向かって走るオトガイ筋の作用に由来するのではないのです。オトガイ筋の付着部はここです。そこから下唇の皮膚へと下方に走向します。したがって、メンターリス・ハビット(オトガイ筋習癖)で観察される皮膚の皺は、今ここで問題となっている下唇溝の緊張とは別問題です。その点を分けて考えてもらうよう、彼らにこう伝えました―「口輪筋や下切筋(口角下制筋)の作用とも思われますが、とくにここでは水平に走向する筋束が問題です。これは下唇方形筋と呼ばれます。ここに対して処置を行って頂きたいのです。」 カニンガム医師の報告では、白人人口のおよそ 1/4 で左右の下唇方形筋の筋束が連続しているそうです。それがオトガイの膨らみを相対的に強調させています。
先に述べた「左右の筋束が連続することで生じる問題かもしれない。」を思い出して頂けませんか... 筋肉の肥厚化こそが問題だからです。この帯状の堅い部分を指でつまみ上げて頂けると、Ⅱ級 2 類や、ときには I級の患者においても、堅い筋束が感触して頂けると思います。喩うなら、ここに重量挙げの力持ちが身構えているようなものです。右左の繊維が結ばれる形で、それが緻密な結合組織となってここを走向していると考えら れます。
オトガイ形成術を行う患者が、ちょうど一人いました。この話を長らく形成外科医に伝えていたので、そのときの担当医ヘンリー・カワモト氏は、手術の最中に「ちょっと見て下さい。あなたがお話なさっていた筋束ですか?」と尋ねてくれました。カワモト氏と私はともに多くの仕事をしてきた仲です。我々はその患者の口唇全体を剥離し、次に下唇を翻転してみることにしました。その瞬間、私は叫びました... 「ここにあった!」 すかさず彼は「ここの処置を行うのですね。」と訊き、「その組織を切除してもらえませんか?」と伝えました。剥離した後、肥厚組織を摘出しました。 彼は私の希望を叶えてくれたのです。したがって第一号患者は、この部位の口唇がきつく引き締った(深い下唇溝)オトガイ前方形成術の患者でした。オトガイ前方形成術を受けた患者でも(このような処置を行わなければ) 強固な窪みが残ったままです。これはあなたも経験されていることでしょう。したがって、オトガイ形成術を行う場合には、下唇方形筋に対する付加的な処置が必要となる場面もあります。これをかわぎりに今まで 90 症例を経験しました。
〔M.〕 Interesting.
〔M.〕 興味深いお話ですね。
〔R.〕 So to release that, instead of treating the teeth to the tight lip, do something about the lip so that you can go ahead and unfold a denture and have a great smile.
〔R.〕 基本的な考え方と致しましては、「きつく引き締まった口唇に 歯を動かのではなく、問題のある口腔内環境に対して何らかの改善アプローチを行った後、そこへ歯を動かす」ということです。こうして、豊かな広がりをもつ歯列が遺憾なく表現される、そんな素晴らしい笑顔を我々は提供できることになります。
〔M.〕 Can you just very briefly describe the procedure?
〔M.〕 術式について、要点を解説して頂けますか?
〔R.〕Yeah. We will go in the sulcus. First of all, we will give an injection just by infiltration of one or two ampoules — one and a half ampoule - all the way around so that we go all the way out to the mental foramena. We don’t go into the mental foramena. We just give a good infiltration for two reasons. Number one, we have epinephrine in it, so we’ll control a little bleeding with it.
Then after that’s taken, we will go in and make an incision right at the midline, right across the raphe. An incision that’s about twelve millimeters long. We then will go in with the periosteal elevator, and we’ll lift the mentalis attachment right off of the little fossas on either side.
There’s a little fossa there and a little ridge on the mandible that you’ll see. A little transverse ridge at the symphysis, almost immediately lateral to the protuberance menti, just a little bit above it. So we’ll go in and elevate that. And then we’ll proceed out to the upper border of the mental tubercles on either side. Now below that is the triangularis right here at the mental tubercle. Right along here is the quadratus origin. And it comes up and comes in here.
So what we want to do is to take that down and free that up.
Now once we do that, then we can lay the lip out quite easily. And we can see, then, the integument of this part of the lip. And we’ll examine it and most of the time we will see a yellowish whitish raphe that is much bigger than it is in the typical case. So we will go in and take that out. And then with experience, excise a little bit to the lateral, particularly in males, and loosen that lip up. Close it up. And that’s the procedure.
〔R.〕 了解しました。まず、下唇溝の内側へアプローチしますが、そのまえにエピネフィリン入りの局所麻酔液を 1 〜 2 本、1 本半位でしょうか、周辺を含めて浸透させます。オトガイ孔には注射しませんが、その領域の近傍までしっかりと麻酔処置を施します。こうしてエピネフィリンの末梢血管の収縮作用で出血を抑える対策も事前に講じておきます。
その後、正中から切開を始め、ここの縫線まで粘膜を切り開きます。切開線の長さは、およそ12mmです。その後、骨膜剥離子を用いてオトガイ筋が付着する左右の小さな窪み部分の繊維を剥離します。
下顎骨をよく観ると、そこには小さな窪みと隆起があります。事前に解剖書や乾燥骨で参照しておいて下さい。下顎正中結合部にある Pm(オトガイ隆起)のすぐ脇に、小さな水平隆起が僅か上方に観察されるでしょう。そこも剥離します。そのままオトガイ隆起の上縁まで左右の剥離作業を進めます。さてここまでくると、その下には三角筋(口角下制筋)が見えてきます。オトガイ結節の辺りです。そこが下唇方形筋の付着している領域です。この筋肉は上へ向かった後、ここに至ります。
我々が意図する処置は、それを下へ剥離し、自由にさせることです。ここまで処置が進んでくると、容易く下唇が翻転できることでしょう。口唇のこの部分における被膜構造も観察することができます。多くの場合、 そこには黄色をおびた白色の縫線が観察されます。通常の患者に比べればはるかに厚みを帯びています。そこからさらに進入し、この部の組織を剥離します。ここからは経験的な判断に基づきますが、僅かに切開をすすめます。とくに男性においては、この処置が必要となります。その後は、唇を楽に翻転させることができます。口唇を元に戻し、粘膜部を縫合し処置は完了となります。
 |
 |
第18回 An Interview with Dr. Robert M. Ricketts 1987
2017.07.26
第18回:Growth Direction 成長方向と歯列安定
An Interview with Dr. Robert M. Ricketts DDS, MS April 13, 1987
Copyright © 2015 University of Michigan School of Dentistry
Some rights reserved. Except where otherwise noted, this work is licensed under the following:
Attribution: Please attribute the work to the University of Michigan School of Dentistry and any individual author(s) cited. Not-for-profit: Use, display, and redistribute all or part of this work for non-profit and educational purposes only.
Share alike: Redistribute derivative works with the license listed here.
Visit the University of Michigan School of Dentistry’s website at http://www.dent.umich.edu/.
View the original interview at https://www.youtube.com/watch?v=lcBLmVOn3m0.
Interview conducted by James McNamara, DDS, MS, PhD. Interview transcribed by Yuri Shindo, MD.
Interview translated by Katsuyuki Shindo, DDS, PhD.
【 Growth Direction 】
〔M.〕 You think that a latent mandibular growth can have something to do with lower incisor crowding?
【 成長の方向と歯列安定 】
〔M.〕 思春期にみられる下顎の潜在的な成長もまた、下顎切歯の叢生を引き起こすと考えられますでしょうか?
〔R.〕 Particularly if it’s vertical.
〔R.〕 とくに垂直的な成長が生じた場合です。
〔M.〕 Why vertical? Because then the -
〔M.〕 なぜ垂直的なのですか? というのも…
〔R.〕 Well, let’s do this geometrically. If I have an occlusal plane here — well let’s see if I can draw my hands maybe for the audience here. Now, let’s say that this is the lower incisor and this is the mandible. Now, with normal growth, this thing is kind of doing this, isn’t it? Okay. Now let’s say that we have late growth and the patient is growing vertically. Now as the mandible is growing, it’s tipping the lower incisors out. If it grows like this, the occlusal plane is doing this. It’s throwing the lower incisors against the lip and the lip is going be increased in tension. And now it’s going to break up front.
So if you have late growth, and particularly if it’s vertical, then you’re going to have this kind of an environment right against this part of the lip, which is a disaster in a case like that. And that’s the reason why, in these vertical growth patterns, you’re obliged to extract sometimes even with a good lower arch. This is what’s ahead for that case. And here you have the vertical growth taking place, more denture height developing, lip strain, and teeth being thrown against it. And you have to use your imagination and you have to see cases in which this takes place. But once you get that, it’s very clear that that’s a possibility. So that’s another modality of crowding.
〔R.〕 一寸お分りにくいかもしれませんので、幾何学的に説明いたしましょう。ここが咬合平面です。聴衆から見ると逆にこうやった方が良いのかもしれません。私の手を見ていて下さい。ここが下顎切歯、ここが下顎骨です。正常な成長はこのように進みます。お分かり頂けましたか? では、晩期的な垂直成長が起きたとしましょう。このようになります。すると、下顎前歯は口唇の筋肉の壁に突きあたるように傾斜していきます。咬合平面も当然傾いていきます。(垂直的に成長すると)余計に下顎前歯は口唇の領域に放り込まれるようにして異常な緊張を受けるに至ります。そして、歯列前方の配列は崩れ始めるのです。
したがって晩期成長でも、とくにそれが垂直的に生じた場合には、 唇の緊張によってこのような力学的な環境がもたらされるのです。これは、 悲劇的な状況といってもよろしいでしょう。下顎の歯列が良好なアーチ形状を保っていたとしても、このような垂直型の成長では抜歯処置を選択することすらあり得るのです。治療開始前にあらかじめ考慮しておくべき事柄でしょう。垂直的な成長が生じて、歯列の高さ (denture height) が増していき、口唇の緊張が増し、そこへ歯列が放り込まれる状況です。皆さんも想像を働かせて、このような現象が起きている症例を観察してみて下さい。ひとたび(垂直成長や筋肉バランスが歯列に与える影響が)理解できますと、その可能性をあらかじめ予知することはさして難しくはありません。これが、従来型とは異なる叢生が発生する機序です。
〔M.〕 Right. Sort of a related question. And I’m sure, if you like me, you’re asked this question every time you open your mouth. Somebody says, “What do you think of second molar extractions?”
〔M.〕 その通りですね。これに関連した質問ですが、下顎第二大臼歯の便宜抜去法について、いかがお考えでしょう。勿論、ことあるごとに「第二大臼歯の抜歯についてはどうですか?」と、あなたは尋ねられているとは思いますが…。
〔R.〕 Well, I did it in my daughter [son]. I did it in my wife. I think it has a place, but to have it as a substitute for third molar enucleation... If I had had the possibility of taking the third molars out in an enucleated way, as far as I’m concerned, there’s no comparison. Because a lot of times the occlusion you end up with, that third molar a lot of times, if you take out four second molars, the upper third is going to come in faster than the lower. That’s pretty well-known.
Okay. Now, that comes down in here. The third molar then has to close up all of that space. It has to already be upright, and a lot of times it’s leaning forward, the occlusal plane is down. And so you don’t get a real good occlusion with the third molars when you take out four second molars, unless you go in and treat it at a late stage. So I’m not saying that it doesn’t have its place. But to use that as a substitute for bicuspids [extraction], to use that as a substitute for the philosophy of “mandibular posturing”and“bone growing”and all of this, I don’t buy it. I think it has a place and I’ve done it, but I think the other modalities we have are superior to it.
〔R.〕 私は自分の(息子)と妻の下顎第二大臼歯を抜去して、第三大臼歯を歯列に誘導する処置を行いました。ふたりとも第二大臼歯根の遠心根が損傷していたので、長期的な視野からこのような処置を選択したのです。したがって確かに必要な場面はあるでしょう。でも、第三大臼歯の歯胚摘出の代替処置に行うというのは… 仮に第三大臼歯を歯胚摘出が可能な状況にあったとしたら、私自身、それとこれとを同じ次元で論じてはならないと思います。なぜなら、4本の第三大臼歯を抜去した場合には次のことが起こってくるからです… 第三大臼歯の萠出速度を上下で比べると、上顎歯の方が早いことはよく知られています。
おわかりでしょうか? さて、上顎第三大臼歯がここまで降りてきたとします。下顎第三大臼歯は抜歯スぺースも閉じるためにここまで移動させてこなければなりませんが多くはアップライトを必要とする形になっているでしょう。実際にも近心傾斜しています。上下の第三大臼歯が噛み合う場所は、手で示しているように咬合平面より下へさがってしまいます。つまり、動的な処置の終わりの段階でここを整えないと、不完全な噛み合わせに落ち着くことになります。第二大臼歯の抜歯法が、選択肢として全くないというわけではありませんが、小臼歯抜歯法の代わりに行う考え方や、学派によっては「下顎ポスチャリング」あるいは「成長促進術」など呼んでいる治療法の代替処置として上下左右の第二大臼歯を抜去するといった臨床に対して、私は全く賛同できません。したがいまして第二大臼歯を抜歯して処置を行った経験が私にもあるとはいえ、我々の行う下顎第三大臼歯の早期歯胚摘出術の方がはるかに優れていると考えています。
 |
 |
 |
第17回 An Interview with Dr. Robert M. Ricketts 1987
2017.08.08
第17回:The Third Molar 下顎第三大臼歯
An Interview with Dr. Robert M. Ricketts DDS, MS April 13, 1987
Copyright © 2015 University of Michigan School of Dentistry
Some rights reserved. Except where otherwise noted, this work is licensed under the following:
Attribution: Please attribute the work to the University of Michigan School of Dentistry and any individual author(s) cited. Not-for-profit: Use, display, and redistribute all or part of this work for non-profit and educational purposes only.
Share alike: Redistribute derivative works with the license listed here.
Visit the University of Michigan School of Dentistry’s website at http://www.dent.umich.edu/.
View the original interview at https://www.youtube.com/watch?v=lcBLmVOn3m0.
Interview conducted by James McNamara, DDS, MS, PhD. Interview transcribed by Yuri Shindo, MD.
Interview translated by Katsuyuki Shindo, DDS, PhD.
【 The Third Molar 】
〔M.〕 Now, one of the other things that you have talked about for some time is third molars. And I know that you have advocated in the past the early enucleation of that. Do you want to talk about third molars from the point of view of early treatment, and also from the point of view of its relationship or lack of relationship to lower incisor crowding?
【 下顎第三大臼歯 】
〔M.〕以前、第三大臼歯のことについてお話をして下さいましたが、過去には、下顎第三大臼歯の早期歯胚摘出術を提唱していらっしゃいましたね。早期治療の観点からご説明を頂けますか? また、下顎前歯部における叢生へ影響するかどうか、それについてもご意見をお聞かせ下さい。
〔R.〕 Okay, let’s start from the beginning again. This idea of third molar crowding has always been controversial. It’s no longer controversial with me. I no longer have any doubts about it. And maybe I can explain it.
So I have been mindful of third molar problems through my experience with TMJ. It’s ironic to me that Brodie opposed extraction tremendously, as did Atkinson. But they recommended third molar removal, just at the slightest provocation. I don’t know if you knew that.
〔R.〕分かりました。経緯からお話しましょう、ご理解の便宜でしょうから。第三大臼歯によって叢生が起こるかどうかについては、昔から論議が絶えませんでした。しかし私の中では疑いの余地は全くなく、「影響あり」とみています。その理由も説明できます。
そもそも顎関節症を患った患者の治療経験から、第三大臼歯の関与ははるか以前から気にかかっていたものです。しかし、皮肉なことにブローディ教授は、第三大臼歯の抜歯処置について強力に反対していました。スぺンサー・アトキンソン氏も同様の見解でした。しかし、(もっと 早い時期 に行う)第三大臼歯の摘出に関しては、医学的にみた誘発試験の範疇とし ては容認されるものとして、彼らは推奨していました。ご存じかどうか知りませんが…。
〔M.〕 No.
〔M.〕 知りませんでした。
〔R.〕 And so third molars were nothing to these people“. Take them out.”So this was a part of the discipline that I experienced very early. Now in [1950], Spenser Atkinson brought his barrels of skulls to Lexington, Kentucky. The national meeting of the American Association was there. And in fact, that was the first time that I was on the national program. I might depart a little bit from the third molar. I got up to give that paper, and if you can believe it, my mouth went dry and I couldn’t say a single word.
〔R.〕 したがって、彼らにとっては第三大臼歯の存在(矯正歯科処置に関連して摘出するかどうか)は問題意識にすらのぼっていなかったわけです。これが、私が臨床を学び始めた頃の教育でした。さて、1950 年のケンタッキー州のレキシントンにスぺンサー・アトキンソン氏はたくさんの頭蓋骨を持参してきました。アメリカの国内学術大会がそこで開催されたのです。この学会は初めて私が経験した学術発表(演題:顔面形状ならびに不正咬合別に観察された顎関節の特徴)でもありました。
話題から少しはなれますが… その時の出来事を皆様にご紹介しておきましょう。じつは緊張のあまり口中が渇ききってしまい、一言も話出すことができない有り様でした。
〔M.〕 I can’t believe that for you!
〔M.〕 本当ですか? 今のあなたからは想像もできません。
〔R.〕 Isn’t that unbelievable?
〔R.〕 信じられませんか?
〔M.〕Sure.
〔M.〕 本当ですよ。
〔R.〕 I got up there and I could not open my mouth. Can you believe that? Maybe that would be good for these students to know about. Despite how much speaking I have done, and my complete lack of concern of getting up in front of almost any audience today, when I started, I couldn’t open my mouth. And I had to look down in the audience. My wife was there, and I said, “Help me Patty.” Isn’t that something? .
〔R.〕 演台に立った途端、口も開かない状態でした。惨めなものです。ここにいる生徒さんたちには、こんな未熟な経験を知って頂くのも悪くはないでしょう。話すべきことが山のようにあったのに、今ここにいらっしゃる皆さんと同じような聴衆を前にした途端、精神は全く集中を欠き、一言も喋ることができなくなったのです。檀上から聴衆を見渡すと妻のパトリシアが座っていました。心の中で叫びました…「助けてくれ、パティ。」 そんなこともありますかね?
〔M.〕 Yeah, it shows that you’re human.
〔M.〕 人間性の一面というものでしょうか。
〔R.〕 So that was [1950]. And I was going along studying Atkinson’s skulls. And I was the only one who was in the room. So he came along and followed me. He picked up a child’s skull and he said, “Look at this. Look at that third molar. Look where it is. Now if you can get in there and enucleate that developing third molar (which was right on the level of the occlusal plane, and it was lying in a cup on the side of the mandible, and even closed lying on the surface). Now if you can get in there and take that out at this time, you’d have no lower third molar problems.”That was in [1950]. So that stayed in my brain for many years.
Then as we came along and we began to get into early treatment, particularly mixed dentition in which we were intruding the lower [molars], we begin to see the lower molar back up. I mean bodily move back. And if the treatment was severe, it would tip back. So now we have the second molar, the first molar over the second molar, and the third molar out up here. So we were impacting second molars with that treatment. Now, not a lot. And once in a while you’d get in trouble. So here I kept looking at that third molar there all this time.
Now we come along in 1970, and I finally discovered this arc. And I said, “Now I’ve truly got a long-range forecast.” And we begin to see the order that the occlusal plane took to Xi point, and we could predict how the lower occlusal plan was going to develop. Well that did it. That gave me the confidence, then, that I could predict where the third molar is going to be, whether it’s going to be impacted or not. Certainly, manually I could do it.
And then I went back and took a lot of the cases that we had done previously. And I said, “Can I predict that we’re going to have a “molar make”or a“molar go”in this case?”And I found out with the study that I did, that about 95 % of the third molar impactions were predictable.
Now once I could do that, then the next thing was the technique of doing it. So I looked around for several surgeons. No, they didn’t want to touch it. They said, “Well, let’s get some animals, let’s do some studies.”I said, “Oh hell! I don’t want to bother with that. I know where it is. Can you do it for me?” “No, I don’t want to mess around. I don’t want to cut into those kids.”
So I kept being frustrated about the whole thing. So one day I told my girl to schedule the third molar enucleation. Busy afternoon. Here I had this patient scheduled. I had forgotten all about it. I had no technique, no nothing. I didn’t even have any tools. So, I said,“ Okay, let’s go!” In the meantime, I had picked up a technique with the electric cautery and I had worked with that. So I said, “Here we go!”
So I knew where it was supposed to be. So I took the — what do you call it… it’s not cautery. Electric cautery machine? Well, it’s cautery but it has a different name. What do you call it? Well, you know what I mean. Anyway, I made an incision there, and I had periosty elevators. I elevated a little bit. “How am I going to get this butt out of there?” So I looked around at my tools, and I had nothing but a wax spatula.
Okay. So I went over and burned the wax spatula, got it all sterilized. And took a pair of pliers, bent a hooked on it. And I made an enucleation with the wax spatula. It was the first one I did. And it was uneventful, everything went fine. I haven’t gotten any tools any better since! It was just a scoop.
So I started doing third molar enucleations. Well, I did several myself and then I showed the technique to a couple of surgeons locally. And they said, “Well, hell, I can do that. If you give me the diagnosis, why, I’l l do it for you.” So I suppose several hundred — I don’t know how many, I’ve lost count. I kept track in the beginning. The beautiful part of it is that in your mixed dentation cases, you no longer worry about impacting second molars.
〔R.〕 1950年の出来事に戻ります。私はアトキンソン氏が持参してきた頭蓋骨をじっくりと調べていました。部屋に居たのは私だけです。しばらくすると彼があらわれ私の後ろをおもむろに歩き、小児の頭蓋骨を手にとると、「これをご覧下さい。第三大臼歯のある場所です。もしこの時期に発達中の第三大臼歯を摘出することができれば良いのではないでしょうか? 咬合平面の高さに位置しており、歯胚を納れるカップ状の窪みの中にあって表面のすぐ下に位置しています。ここに切開を入れて器具で到達することができれば、もうこれ以上、あなたは下顎第三大臼歯の問題に悩まされずに済むでしょう。」この 1950 年の出来事は私の記憶に深く刻まれました。
その後、早期治療の可能性に次々と挑み、とりわけ混合歯列期で下顎の前歯を圧下移動させると、下顎大臼歯が後方へ潜り混んでしまう現象に気づきました。それは、傾斜ではなく歯体移動でした。治療が困難になればなるほどより多くのアーチレングスの獲得に努めなければならないので、遠心へ傾斜してしまいました。さて、第二大臼歯がここにあり、第一大臼歯がここまで下がってきますが、第三大臼歯はこの上に位置しています。となれば、このような術式では第二大臼歯がインパクションを起こしかねません。頻度としてはさほどではなくても、ひとたびこれが起これば、その後は治療がたいへん困難となります。そのようなわけで、当時は第三大臼歯の位置とその動向に注意を払っていたのです。
1970年、私はこのアーク状の成長をようやく発見、「ついに本当の長期成長をとらえたぞ!」と叫びました。これが突破口となるや否や、機能咬合平面が Xi ポイントの近傍を通過する特徴や、下顎の咬合平面(※ 下顎咬合平面が咬合平面を決定する主要素)の発育の様相まで予測が出来ることも分かってきました。実際、そのように下顎の成長は振る舞うのです。これに自信を得てからというもの、第三大臼歯の萠出の位置、あるいはその埋伏の有無も分かるようになってきました。勿論、手作業で成長予測を行っていた時代のことです。
次に、以前治療した数多くの症例についても検討を加えてみることにしました。「このケースでは、大臼歯は生えることができるか、それとも抜く運命にあるのか?」などと、自分に呟きながら進めました。この研究を通して、下顎第三大臼歯の埋伏を、とうとう95%の予知性を以て推定できることが明らかとなったのです。
れました。
その後、早期治療の可能性に次々と挑み、とりわけ混合歯列期で下顎の前歯を圧下移動させると、下顎大臼歯が後方へ潜り混んでしまう現象に気づきました。それは、傾斜ではなく歯体移動でした。治療が困難になればなるほどより多くのアーチレングスの獲得に努めなければならないので、遠心へ傾斜してしまいました。さて、第二大臼歯がここにあり、第一大臼歯がここまで下がってきますが、第三大臼歯はこの上に位置しています。となれば、このような術式では第二大臼歯がインパクションを起こしかねません。頻度としてはさほどではなくても、ひとたびこれが起これば、その後は治療がたいへん困難となります。そのようなわけで、当時は第三大臼歯の位置とその動向に注意を払っていたのです。
1970年、私はこのアーク状の成長をようやく発見、「ついに本当の長期成長をとらえたぞ!」と叫びました。これが突破口となるや否や、機能咬合平面が Xi ポイントの近傍を通過する特徴や、下顎の咬合平面(※ 下顎咬合平面が咬合平面を決定する主要素)の発育の様相まで予測が出来ることも分かってきました。実際、そのように下顎の成長は振る舞うのです。これに自信を得てからというもの、第三大臼歯の萠出の位置、あるいはその埋伏の有無も分かるようになってきました。勿論、手作業で成長予測を行っていた時代のことです。
次に、以前治療した数多くの症例についても検討を加えてみることにしました。「このケースでは、大臼歯は生えることができるか、それとも抜く運命にあるのか?」などと、自分に呟きながら進めました。この研究を通して、下顎第三大臼歯の埋伏を、とうとう95%の予知性を以て推定できることが明らかとなったのです。
つぎに、順番として問題になるのが、歯胚や歯冠を摘出する実際の術式です。そこで協力してもらそうな口腔外科医を探し回りました。しかし、手術に前向きな人は誰もいません。口を揃えて彼らは、「動物実験をまずは行ってご覧になり、有効性を確かめた後に行いましょう。」と言うばかりでした。… それでも私は諦めず、「ご迷惑をお掛けしませんから行ってもらえませんか。どこにあるかも分かりますので、助けてもらえませんか?」と尋ねてみました。でもやはり答えは同じく「残念ですが、協力は致しかねます。とりわけ、子どもたちにメスを入れるなんて躊躇せざるを得ませんので。」と突き返されてしまいました…。
予測ができても実践の手立てがない、私自身大きなストレスを抱え込んでいました。悶々としていたある日、スタッフの女性に下顎第三大臼歯の摘出術の予約を入れるよう伝えました。当日は多忙な午後、いよいよ手術とは言っても予定を入れていたことすらすっかり忘れていました。術式としてこれといった持ち合わせはなく、何を揃えていいかも分からず、特別な器具の準備がないまま歯胚の摘出に挑むことになりました。「よし、いくぞ!」とスタッフにも気合いを入れました。その頃、電気焼灼器を用いた手術法を普段の臨床に取り入れていたので、「場所は定まった!」と 自分に言い聞かせ、およその位置に見当をつけて切開を入れました。電気焼灼器を正式には何て呼ぶのでしょう、まぁ、良いでしょう。意味が通じればそれで構いません。とにかく切開の後、骨膜を剥離し、歯胚を少し持ち上げました。「さて、ここからどうやってこいつ(歯胚)を摘出したらよいものやら?」… あたりを見渡すと、ワックススパチュラが目に飛び込んできました。直感的に「そいつなら行ける!」と判断し、スパチュラを手にとりバーナーで加熱滅菌、プライヤーで掴んで良さそうな案配に曲げ、歯胚があると思しき場所へそいつをひっかけました。一回目の歯胚摘出はなんとワックススパチュラで行ったのです。面倒なことは何一つ起こりませんでした。以来これに勝る外科器具に出会ったことはありません。「ひしゃく」と呼んだ方がいいでしょう。
これを機に、下顎第三臼歯の歯胚摘出をはじめました。地元の二つの口腔外科医グループにも、この術式を教えました。「これなら私にもできる! もしあなたがきちっと診断して下さるなら私が歯胚をお取りしても良いですよ。」… 今度は前向きな姿勢を見せてくれるようになりました。それから、数百症例の手術を経験しましたが、当初は症例数を数えていたものの途中からは数えるのも忘れました。混合歯列期にこのような処置ができれば、下顎第二大臼歯のインパクションに悩まされる心配はもうありません。
〔M.〕 Your second molar will go distally?
〔M.〕 下顎第二大臼歯が遠心に移動していくのですか?
〔R.〕 Oh, it will fill half of the space. The second molar will erupt distally right up into the crypt where the third molar was enucleated.
〔R.〕 第三大臼歯の歯胚を摘出したスペースの半分程度まで、自然 に遠心へ動いてくれます。下顎第二大臼歯は歯囊のあったところ(歯胚洞) へ遠心に向かって萠出します。
〔M.〕 Now you said before — just to have you articulate what you’re thinking. What do you think the role is of the third molar with regard to —
〔M.〕 以前、あなたは「思考を整理するのはご自分ですよ」と説いていらっしゃいました。混乱した意見に混乱した学説が重なっている第三大臼歯の役割について、どうかご意見をお聞かせ下さい。
〔R.〕 Number one, I’m not promiscuous with their removal. I think everybody should understand that. That anything that is not more than maybe in the range of only a 30% to maybe 35% probability. In other words, I have to have about a 70% probability of impaction before I’ll enucleate. So I think I’m pretty careful. I mean, that gives me a 20% margin. And as far as I know, I’ve never made a mistake yet with it. Maybe one little black girl. Maybe. She had a tremendous amount of growth in the mandible. And I’d taken teeth out on her for a double protrusion.
〔R.〕 第一に大切なことは、むやみやたらに摘出を試みるようなことがあってはならない、ということです。いい加減な予想や期待は慎まなくてはなりません。すべての臨床者が心得ておくべき基本です。30〜35%の萠出の可能性、言い換えれば 70%の確率性をもって埋伏が予測される場合、あるいはもっと高い割合で萠出余地の不足が予測される場合は、歯胚摘出を実施するのに差し支えはないものと私は判断します。しかしより慎重に構えて、20%しか萠出の可能性が見込まれない場合をもって、境界線と考えています。私は見通しを誤ったことはありません。ただもしかしたら黒人の少女の一症例については、判断に狂いがあったかもしれません。彼女は成長につれて、とてつもなく旺盛に下顎が発育していきました。診断当初は、上下歯列前突の是正として第三大臼歯の歯胚摘出を計画していたのですが…。
〔R.〕 I do believe that the third molar has a function, not like a lot of people think, but I think it helps with“the curve of Spee”, holding the condyle back in centric. And I think it adds to the vertical support of the face. So I think that it can - you know it’s a tooth after all. And if it can be in and in function, then it’s of benefit to the occlusion. So I’m not promiscuous with it. But on the other hand, I do believe that when it doesn’t have enough space, it’s going to make itself known. It’s going to, particularly if it comes in at an angle, which it does, and it starts to erupt, it’s going to have a force that’s going translate right down the occlusion.
I not only believe that, but I believe it can be measured. If we abstract that out in terms of the intrusion force that we know takes it, calculate that on the base of the root, the force of a third molar can have as much as 25 grams of force coming down the line of occlusion on both sides. That’s 25 grams a side.
it. Maybe one little black girl. Maybe. She had a tremendous amount of growth in the mandible. And I’d taken teeth out on her for a double protrusion.
〔R.〕 第一に大切なことは、むやみやたらに摘出を試みるようなことがあってはならない、ということです。いい加減な予想や期待は慎まなくてはなりません。すべての臨床者が心得ておくべき基本です。30〜35%の萠出の可能性、言い換えれば 70%の確率性をもって埋伏が予測される場合、あるいはもっと高い割合で萠出余地の不足が予測される場合は、歯胚摘出を実施するのに差し支えはないものと私は判断します。しかしより慎重に構えて、20%しか萠出の可能性が見込まれない場合をもって、境界線と考えています。私は見通しを誤ったことはありません。ただもしかしたら黒人の少女の一症例については、判断に狂いがあったかもしれません。彼女は成長につれて、とてつもなく旺盛に下顎が発育していきました。診断当初は、上下歯列前突の是正として第三大臼歯の歯胚摘出を計画していたのですが…。
〔R.〕 I do believe that the third molar has a function, not like a lot of people think, but I think it helps with“the curve of Spee”, holding the condyle back in centric. And I think it adds to the vertical support of the face. So I think that it can - you know it’s a tooth after all. And if it can be in and in function, then it’s of benefit to the occlusion. So I’m not promiscuous with it. But on the other hand, I do believe that when it doesn’t have enough space, it’s going to make itself known. It’s going to, particularly if it comes in at an angle, which it does, and it starts to erupt, it’s going to have a force that’s going translate right down the occlusion.
I not only believe that, but I believe it can be measured. If we abstract that out in terms of the intrusion force that we know takes it, calculate that on the base of the root, the force of a third molar can have as much as 25 grams of force coming down the line of occlusion on both sides. That’s 25 grams a side.
I had two cases in my career, actually three now, in which I had four-to-four retainers on. And it’s not going to crumple these teeth here. The third molars started in, and it buckled the second bicuspid to the lingual. I took the third molars out, and the second bicuspids went back into position with no orthodontic treatment.
〔R.〕 第三大臼歯の機能について、私は他の臨床家が考える内容とは違った重要性を信じています。第三大臼歯はスピーカーブの後方に位置している関係上、下顎頭が関節窩におさまるのを安定させてくれる役割を担っています。さらに、顔そのものの構造を後方から支持する働きもあります。したがって、もしきちんと生えて機能することができれば、咬合にとって誠に有益です。でも… もっと素朴に考えてみれば、もともと第三大臼歯も体の一部です。ですから、再応、歯胚の摘出は慎重にならざるを得ないのです。しかし一方において、萠出に足りるスぺースが得られないとなれば、とりわけ傾斜や埋伏といった状況に陥って萠出力が下顎歯列にまともに加われば、噛み合わせは足もとから崩される危険がある、そう私は確信しています。
このような現象の起こる可能性をただ漠然と信じているのではありません。力の大きさも計測できます。歯の萠出力については(※ 日本の三浦氏を始めとする諸研究を参照)歯根の単位面積あたりの萠出力と圧下移動を起こさせる力まで分かっているので、第三大臼歯の萠出力を逆算的に推定することができます。このような角度で押してくるとすれば、下顎歯列の咬合ラインに沿って片側 25g の力を発揮してくるでしょう。片側 25g です。
今までに2症例、最近の例を加えると3症例になりましょうか、下顎第一小臼歯間の舌側にわたした保定装置(※ 左右第一小臼歯にバンドを装着、舌側にコバルトクロムのワイヤーがろう着されているタイプのバンド合着式保定装置)をつけた患者で興味深い現象を見出しました。下顎第三大臼歯が生えてくると、頬側に揃っていた第二小臼歯が舌側に傾いてきたのです。第三大臼歯を抜去したあと、なんとその歯が元の位置へ自然に復帰したのです。
〔M.〕 Interesting.
〔M.〕 実に面白い現象ですね。
〔R.〕 How would you - I mean I’m a farm boy and I’ve looked at a mule’s rear end for long years and I think that’s common mule’s sense! That if you have a patient like that, that’s pretty good evidence to me that a third molar has been the culprit in that situation.
So I don’t have any doubts at all anymore that the third molar can cause a break in the lower arch. Too many cases clinically — you’ve seen happen. Even in patients who had normal occlusions. And people say“, What about those cases that break when there is no third molar present?”Well, what about that? It doesn’t mean that the third molar is the only force. The first molar and the second molar are still in there operating. The third molar is just adding to the whole mesio thrust.
〔R.〕 どう思いますか… 農場育ちの私は、小さい頃からずっとラバの尻を見て育ってきました。ラバは知識張らず頑固にじっくり構えて行動するので愚鈍と罵られますが、しまいには経験がものを言う喩えです。第三大臼歯が引き起こす問題をこうして述べているのも、私独自の感覚やら経験の産物ですよ。もし、そのような症例をあなたも経験されることがあれば、私が感触している第三大臼歯の関与を見事に証明してくれたことになるでしょう。
そのようなわけで、下顎歯列が崩壊するひとつの誘因として、この歯の関与は私にとってはもはや自明の理です。ご存じの通り、臨床ではあまりにも頻繁にこの問題へ我々は直面します。今まで正常咬合だった人が(第三大臼歯の萠出やら埋伏したまま動こうとする力が契機となって)、歯がガタガタになってくることもあるわけです。「第三大臼歯がすでに抜去されているのに、どうして叢生が…?」と人々は訝るのですが、何も第三大臼歯だけが近心方向への萠出力をもっているわけではありません。第一大臼歯も第二大臼歯も同様の力を(ベクトルとしては)
〔M.〕 実に面白い現象ですね。
〔R.〕 How would you - I mean I’m a farm boy and I’ve looked at a mule’s rear end for long years and I think that’s common mule’s sense! That if you have a patient like that, that’s pretty good evidence to me that a third molar has been the culprit in that situation.
So I don’t have any doubts at all anymore that the third molar can cause a break in the lower arch. Too many cases clinically — you’ve seen happen. Even in patients who had normal occlusions. And people say“, What about those cases that break when there is no third molar present?”Well, what about that? It doesn’t mean that the third molar is the only force. The first molar and the second molar are still in there operating. The third molar is just adding to the whole mesio thrust.
〔R.〕 どう思いますか… 農場育ちの私は、小さい頃からずっとラバの尻を見て育ってきました。ラバは知識張らず頑固にじっくり構えて行動するので愚鈍と罵られますが、しまいには経験がものを言う喩えです。第三大臼歯が引き起こす問題をこうして述べているのも、私独自の感覚やら経験の産物ですよ。もし、そのような症例をあなたも経験されることがあれば、私が感触している第三大臼歯の関与を見事に証明してくれたことになるでしょう。
そのようなわけで、下顎歯列が崩壊するひとつの誘因として、この歯の関与は私にとってはもはや自明の理です。ご存じの通り、臨床ではあまりにも頻繁にこの問題へ我々は直面します。今まで正常咬合だった人が(第三大臼歯の萠出やら埋伏したまま動こうとする力が契機となって)、歯がガタガタになってくることもあるわけです。「第三大臼歯がすでに抜去されているのに、どうして叢生が…?」と人々は訝るのですが、何も第三大臼歯だけが近心方向への萠出力をもっているわけではありません。第一大臼歯も第二大臼歯も同様の力を(ベクトルとしては)もっていると考えるのが自然でしょう。第三大臼歯が近心方向への力を加算するとみるべきです。
 |
 |
 |
 |
第16回 An Interview with Dr. Robert M. Ricketts 1987
2017.08.01
第16 回:The Concept of Unlocking 内包力を引き出す
An Interview with Dr. Robert M. Ricketts DDS, MS April 13, 1987
Copyright © 2015 University of Michigan School of Dentistry
Some rights reserved. Except where otherwise noted, this work is licensed under the following:
Attribution: Please attribute the work to the University of Michigan School of Dentistry and any individual author(s) cited. Not-for-profit: Use, display, and redistribute all or part of this work for non-profit and educational purposes only.
Share alike: Redistribute derivative works with the license listed here.
Visit the University of Michigan School of Dentistry’s website at http://www.dent.umich.edu/.
View the original interview at https://www.youtube.com/watch?v=lcBLmVOn3m0.
Interview conducted by James McNamara, DDS, MS, PhD. Interview transcribed by Yuri Shindo, MD.
Interview translated by Katsuyuki Shindo, DDS, PhD.
【 The Concept of Unlocking 】
〔M.〕 Again, getting back to my statement before, is it conceivable that by making the maxilla wider, you could theoretically have a slight forward posturing of the jaw?
【 内包力を引き出す 】
〔M.〕 少し前の私の話に戻りますが、上顎骨の側方拡大によって下顎骨が前方に成長を開放されるという可能性も考えられるでしょうか?
〔R.〕 I think so. I think that you’ll get self-activation of the mandible in some children. No question.
〔R.〕 それも考えられるでしょう。小児患者によっては、自発的な下顎骨の成長促進が起こると考えられます。全く同感です。
〔M.〕 I think when I was going through my training, I had heard that in cases involving cervical head gear, many times the clinician would perceive more growth of the mandible. Does that still fall into the same category? Have you seen that?
〔M.〕 矯正歯科の臨床研修を私が受けていた頃、サービカルトラクション(頸部後方牽引装置:H/G)を使うと、いくつかの例において、下顎骨の成長がより大きく発揮される場合があることに気づいた臨床家がいました。これはあなたのカテゴリーに分類される現象でしょうか? 同様の現象をあなたも確認なさっていらっしゃいますか?
〔R.〕 I think that that’s a possibility. I don’t know whether in an interview like this, people fully appreciate the concept of the arcial growth of the mandible.
In the past, we’d always assumed that the mandible was resorbing on the anterior border of ramus and having apposition on the posterior border; the ramus was growing backward; and the body was left out here. Well that just doesn’t make sense because nature is not going to lay down a great oblique bridge here only to resorb it in the next moment. So the mandible actually grows vertically, grows on this arc. And as it does so, this is the part that does the drifting. In here. So the gonial angle drifts around and the apposition then occurs in the top of the condyle, top anterior to the condyle. And this arc, then, is the manner in which the growth is going.
The lower teeth are erupting upward and forward, which actually is the mechanism for the subsequent eruption of the posterior teeth. Now if you can understand that, you can understand why you get a slight extrusion. That’s the reason why I was interested in your technique that you showed me this morning. That’s exciting to me because I’ve been looking for something like that. I didn’t know that you were overlaying your cases.
〔R.〕 可能性の範囲として捉えておくべきでしょう。このようなインタビューの中で、アーク状に回旋する下顎の成長について、すべての方にご賛同頂けるかは分かりません。
過去には、下顎の成長というものは、下顎枝における前縁の吸収と、後縁における骨の添加によって、下顎枝が下顎体に対して後方へ変位していく機序によるものと説明されていました。(※ これはハンターによって提唱(1771)され、ハンフリーによる豚の実験でそれらしき現象が確認され(1838)、イギリスのブラッシュが豚の飼料にレズリンレッドS(染色剤)を含む野菜を与えた 1928 年の成長研究によって補強された)。この考え方には、誤りがあります。下顎体がその位置を維持し、下顎枝のみが後ろに動くという解釈は、頭の中で思い描いたに過ぎません。なぜなら、側頭筋によって吊るされる強靱な構造体である外斜線が、そう容易く吸収していくはずなどないからです。したがって、下顎骨はアーク状に、そして下顎枝は垂直方向に発育するのが自然の摂理です。つまり、この部分はその流れにのるようにドリフトしていき、顎角部も移動し、下顎頭の前方部分は骨添加が促されるといった具合です。このアーク状の成長こそが、下顎骨が発育する様式そのものを表現しています。(このアーク状の成長の中で)下顎の歯は上方および前方に萠出していきます。下顎骨のこの成長は後方歯の萠出に一連して起こるメカニクスです。もし、あなたがこの現象の背景を理解し、その理由も把握できれば、「僅かな挺出」の真意も納得して頂けるでしょう。(私の言った)臼歯部における歯牙の少量の挺出が下顎頭の前上方への成長を促すわけです。これは、今朝あなたからお見せ頂いた治療法について、私が興味を抱いた点でもあります。そのような臨床技法がどこかにないか、私自身模索していたところなので、とても興奮しました。オーバーレイ式の装置にしていらっ しゃるとは知りませんでした。
〔M.〕 The bonded expander?
〔M.〕 ボンド式の拡大装置のことでしょうか?
〔R.〕 The bonded expander. You may be doing a lot more than you realize. My guess is that you’re enjoying the same thing there. Certainly you’re not raping the mandible the way we used to, with the technique that we used.
〔R.〕 そう、ボンド式の拡大装置のことです。論理的な解釈よりも、きっと多くの実践を積んでいらっしゃるのでしょうね。おそらくは同様の良好な結果を得ることとなりましょう。少なくとも、かつて我々が行っていた治療手技で下顎骨を医原的に破壊するようなことは回避されるに違いありません。
〔M.〕 One of the things that I found is that when we do this type of therapy, and the patient is end-on Class Ⅱ, instead of saying, “Well, we will have to do some type of anteroposterior correction,” I say,“We might have to.” And it’s amazing that after a year of doing six months of expansion and six months of just letting them sit with an upper plate, those Class Ⅱ’s just sort of disappear.
〔M.〕 このようなタイプの治療法で、例えば臼歯関係がエンドオンのⅡ級症例に関して、「前後関係でなんとか是正する」というのではなく、「気づけばすでにそうなっていた」というのが、より適切な表現かも知れません。実際には1年の処置… 6ヶ月の拡大と6ヶ月の保定… の間に、上顎のプレート状の装置を装着したまま成長が推移してくると、Ⅱ級関係がおのずと是正されてくる現象を確認しました。
〔R.〕 That’s right. That’s right.
〔R.〕 全くその通りです。
〔M.〕 Where does rapid palatal expansion, the Andrew Hass type of approach, fit into your philosophy?
〔M.〕バンド型装置に拡大スクリューを取り付けたアンドリュー・ハス型の口蓋拡大治療は、あなたの考えに合致していますか?
〔R.〕 I’m a little lost for dates, but I remember when we first started with this. Well, I remember Krebbs and Björk in 1958 when I was there in Europe, showing me their occlusal films. Of course I went back at that time and started experimenting with the jack screw and taking laminagraphs. Rolf Bench was just starting with me at that time, so he got on the circuit and started following closely a lot of the patients that we did rapid expansions with. Bob Worts in Illinois had done a lot of work on that. And I was interested, of course, in the total aspects of it in terms of breathing, tongue posture, growth, and all of the associated things that would occur with it. We used it for about five years, and it definitely became a part of our treatment.
One day I began to go back and analyze the results of the patients we had treated with rapid palatal expansions. And I said“, Wait a minute! Wait a minute! This is no better than what I’d been doing before with the quad helix.”So I made a study - I never published this - but I made a study in about a five-year level of the results of one versus the other. And the ones I treated with the“W”, or the quad helix, came out to be better. It came out to be less work, it was a dirty appliance, and it was hard to get on. You had to separate the teeth, it was a lot of work, and then you had to hold it after you got a split. Then I learned from Storey, who visited me and was my house guest for about a week. He had examined the kind of bone that was present after the palatal split versus the slower expansion, and he found that there was a lot more solid bone that behaved a lot better. The bone was very mushy after you took one of those things off. And you know — you’ve had experience — you take it off and it’s back in about as fast as you expanded it if you’re not careful. So you have to keep it in there for three months.
〔R.〕 いつのことかはっきりと覚えていませんが、たしか 1958 年にヨーロッパに国際学会の演者で呼ばれた際に、クレッブス氏とビョルク氏は(正中口蓋縫合を)咬合法で撮影したレントゲン写真を何枚か私に見せてくれました。折しも私は、ジャックスクリュー式による試験的拡大を臨床に取り入れ、その効果をラミナグラフで確認していました。ロルフ・べンチ氏が一緒に仕事を始めたころで、多くの患者の口蓋急速拡大法について、その効果や安定について研究を手伝ってもらうことにしました。彼は治験症例を注意深く一巡して、資料を集めてくれました。口蓋急速拡大については、すでにイリノイ大学のボブ・ワーツ氏が多くの業績を完成していたので、呼吸、舌の位置、成長といった関連するすべての事柄を総合的に私は検討することにしたのです。およそ 5 年の間、急速拡大法を臨床に取り入れていたので、これはすっかり私の臨床法の一部として定着していました。
ある日、口蓋の急速拡大法を適用した患者を再び調べてみることにしました。そして驚きました… 「待てよ、よく考えてみろ。これは以前 Q/H で治療していた結果に比べて、どこにも優れた点が見当たらないではないか」と。疑問を明かすべく研究に着手しました。その結論については、論著による出版に至りませんでしたが、5年の治験例を追跡調査した結果を端的に述べると、「Q/H やその前タイプのW型装置の方が、ジャックスクリュー式に比べて治療結果が優れており、作業性も良好である」と結論づけられました。4ヵ所にバンドを装着するジャックスクリュー式の急速拡大装置は、清掃性が極めて悪く、装着に至っては至難の技を要する装置です。バンドを合わせる前処置として、歯間部の空隙を広げ、さらに装置を入れるまで隙間を保っておくのも大変な労力であり、正中口蓋縫合が広がった後も新生骨が安定するように、しばらくは入れたままにして置かねばなりません。
折り合いよろしく、オーストラリアのシュトーレイ氏がわが家の客人として 1 週間ほど滞在しましたので、さっそく私は骨生物学者の彼に意見を訊いてみました。彼は口蓋拡大の途中と拡大後の骨の成熟度を、急速スプリット型装置と、緩徐な拡大装置との比較で検討していました。彼の見解によると、後者の方が成熟した緻密な骨が形成されてくるということでした。前者の新生骨は、装置除去後も粥状で脆弱な状態が長く続くそうです。ご存じの通り、急速拡大では注意深く処置をしないと、後戻りがにわかに生じてしまいます。したがいまして、拡大後も3ヶ月間は装置を口の中に装着して置かなければなりません。
〔M.〕 You have to keep an expander in for three or four months.
〔M.〕 3〜4ヶ月も装着しておかなければなりませんね。
〔R.〕 Yeah, that’s right. So in three or four months, where are you? You’re in the same place. You may do it slowly, but I didn’t see any difference in what I had achieved. And who would think that with the upper molar alone — well, with little finger springs against it — that that was enough anchorage to divide a whole palate? Nobody would dream of that, any more than they would dream that an extra-oral head gear pulling back on only the molars could tip a whole palate back. You see? So this was the thing that was hard to explain.
So once I learned that, and once I got efficient at putting it in, it was more economical and easier. I could do intra-oral adjustments with it, I could just clip [the lateral arms] out and put head gear on if I needed it later, or I could put on auxiliary appliances of any kind. So that’s when I left it. And fifteen years, maybe, that I haven’t put a jack screw in. That doesn’t mean that I don’t expand, but the majority of it’s done with the quad helix. And the majority that I would prefer to do is intra-oral adjustments with it if you have the tools and know how to do it.
〔R.〕 その通りです。3〜4ヶ月も治療の進行は止まったままではありませんか。ゆっくりと拡大すれば私が行うのと同じ治療結果を得るわけです。おそらく、左右の大臼歯だけで ― ただし、側方アームが付いていますが ― 口蓋全体を側方へ拡大できる十分なアンカレッジが得られるなどということは、初めて耳にする人にとっては信じ難いかもしれません。ましてや、口腔外牽引装置の力を、バンドを取りつけた第一大臼歯や第二乳臼歯にかけるだけで口蓋全体が後方へ傾斜することなど、想像の域を超えているのではないでしょうか。ご理解頂けましたか? これも人々に納得させるのは大変な苦労でした。
ひとたび、この原理を掴むことができてから、Q/Hの装着は簡単になり側方アームをつまむだけで調整が行えるようになったばかりか、必要に応じて拡大後にバンドを残してQ/Hだけを外し、そこへヘッドギヤーを装着したり、多くの種類の付加的な装置を併用することができるようになりました。これらが診療所の運営にも大きく貢献したことは言うまでもありません。そのようなわけで、ジャックスクリュー式に我々は見切りをつけました。爾来15年、ジャックスクリュー式の適用は皆無となりました。私が上顎骨の側方拡大を行わなくなったのではなく、必要な場合は、Q/Hだけで用が足りるようになったからです。調節用のプライヤーを用いれば、口腔内の調整はいとも簡単に行えますが、調整法を習得しておく必要もあります。
〔M.〕 Now, you’re using a .036 blue Elgiloy?
〔M.〕 0.036 のブルーエルジロイを使うのですか?
〔R.〕 No, .038.
〔R.〕 0.038 inch です。
〔M.〕 .038 blue Elgiloy?
〔M.〕 0.038 inch ですか?
〔R.〕 Yeah.
〔R.〕 ええ。
〔M.〕 Heat-treated or un-heat-treated?
〔M.〕 熱処理の有無についてもお聞かせ下さい。
〔R.〕 Un-heat-treated. Well, you are going to heat treat it a little bit at the attachment, but just soldering it on. So it will be essentially heat-treated right where the burn is.
〔R.〕 熱処理を施さない柔らかいエルジロイです。勿論、ろう着部は熱処理によって硬くなります。ろう着部だけです。どうしてもろう着した際に加熱されるため、そこは硬くなります。
 |
 |
第15回 An Interview with Dr. Robert M. Ricketts 1987
2017.07.26
第15回:The Birth of the Quad Helix クウォードヘリックスの誕生
An Interview with Dr. Robert M. Ricketts DDS, MS April 13, 1987
Copyright © 2015 University of Michigan School of Dentistry
Some rights reserved. Except where otherwise noted, this work is licensed under the following:
Attribution: Please attribute the work to the University of Michigan School of Dentistry and any individual author(s) cited. Not-for-profit: Use, display, and redistribute all or part of this work for non-profit and educational purposes only.
Share alike: Redistribute derivative works with the license listed here.
Visit the University of Michigan School of Dentistry’s website at http://www.dent.umich.edu/.
View the original interview at https://www.youtube.com/watch?v=lcBLmVOn3m0.
Interview conducted by James McNamara, DDS, MS, PhD. Interview transcribed by Yuri Shindo, MD.
Interview translated by Katsuyuki Shindo, DDS, PhD.
【 The Birth of Quad Helix 】
〔M.〕 When I took your course 1974, one of the techniques that you advocated at that time was the quad helix appliance as an interceptive device. Do you want to discuss that a little bit?
【 クウォードヘリックスの誕生 】
〔M.〕1974 年にあなたのコースを私が受講した際、不正咬合の進行を防ぐ早期治療の装置として、Q/Hの説明がありました。これについても解説して頂けますか?
〔R.〕 Well, this started with the old W-appliance. When I was at Illinois, Brodie came to me during my second year and asked me if I would be the orthodontist for the cleft palate program, the Crippled Children’s Service in the state of Illinois. I was a part of the original cleft palate team with Kev Baker, Pruzansky, and the Ear, Nose, and Throat people. He also said, “Do what you can, anything you can, to prevent the mutilation that the surgeons are doing to these cleft palate children.” And he said,“You have absolute freedom to do anything you want to do.”
So I began to look around for techniques and I consulted, at that time, Bill Adams at Indiana. He showed me the original Pollack W-appliance. I didn’t know that Pollack had designed it. I didn’t know where it came from. Pollack later told me that he did, and wrote a paper on it which was titled, “History Repeats Itself”. Do you remember that paper? So he took credit for the W-appliance. Well, I didn’t care who did it, I just didn’t know that he had done it.
So we began to put in this W-appliance, and that was my first inkling that we could do more than move teeth because I was seeing in frontal sections, lamina graphs, and tomograms that we were widening the jaws. That was done in .040 gold, and I was following these later with frontal head films on a routine basis. And I began to find that the palate was widening in patients where I hadn’t worked left. So I could see that this was a possibility.
I then began to modify that with a loop on either side to give it more range, so that I wouldn’t have to make adjustments so much. In the beginning, I’d take out, cement it, adjust it, take it out, cement it... So I was taking it off and re-adjusting and re-cementing it. And I wanted something that I could adjust intra-orally. So I started out with a loop here which gave me more range. And then one day I started using Elgiloy wire. It was too heavy, put too much force, and hurt the teeth. So I reduced it to .038 Blue Elgiloy wire.
Then I said, “Well, why don’t we experiment with another loop?” So that was four loops in it, and I compressed it and measured it. I found out that I could put 600 grams of force, which was enough to split a palate.
The other thing that I didn’t like about the other techniques was that if you have a rotated [molar] forward that you have expanded, you would still have the rotation after you’ve got it expanded. So if I can get something that would widen the palate, rotate the molars, open up the airway, and give rise to space for lingually displaced upper laterals, I would have a good appliance. So that was the birth of the quad helix.
〔R.〕 分かりました。原型は古典的なW型装置に遡ります。イリノイ大の大学院で二年生の時、ブローディ教授から「唇顎口蓋裂患者の治療チームを編成するのでその矯正歯科担当医として加わってもらいたい」と依頼を受けました。イリノイ州の重度小児患者施設における医療活動でした。ケブ・ヘべイカー氏や同期のプルザンスキー氏、耳鼻形成外科医、咽頭外科医とともに仕事をしました。ブローディ教授はこのようにも私に伝えました…「全責任は私がとるから、君が考える最善の方法で、口蓋裂の小児が外科処置後に歯列治療の困難な状況に陥るのを防ぐ手立てをなんとか講じてくれ。」 そのようなわけで、私はいろいろな治療法を探し回り、様々な人に意見を求めました。インディアナ大学のビル・アダムズ氏が、ポーラック氏考案のWアプライアンスを紹介してくれました。ポーラック氏のデザインであったことも、また原型がどこにあったのかも知りませんでした。この装置に関する論文を「歴史は繰り返す」と題して発表したとポーラック氏は後日話していました。ご存じですか?
そのような経緯で、彼はWアプライアンスに高い信頼をおいていました。もとより誰が考え出したかは私にとって興味はありませんが、ポーラック氏が原型の考案者だということです。このようなわけで、試みにこのWアプライアンスを患者に適用しました。正貌断層写真およびトモグラムで調べてみると、Wアプライアンスを使った患者では、口蓋の拡大像が確認されたので、これは単に歯を動かすだけではなく、それ以上の効果があることを、漠然とですが確信しました。使用したワイヤーは、直径およそ1mm(0.040 in.)の貴金属線です。引き続き正貌断層写真による確認作業をルーチンべースで行うことにしました。しかも、口蓋裂の患者以外でも同様の装置を用いて順当に口蓋が広がっていることを知りました。こうして、その可能性の広さを感じ取ったのです。
はじめの頃はバンドを外して調整し、再びバンドを合着するという作業を繰り返していましたが、大変に手間がかかりました。その対策として、 ワイヤーの弾性を向上させ、口腔内でも容易に調整ができるよう、装置のデザインを一部変更、バンドろう着部の後方にループ(Helix)を設けたのです。(金合金に最も物理特性が近いとされる)エルジロイワイヤーが開発されたのを機に、このワイヤーへ変更したのですが、力が過大であったため歯根の損傷を経験し、ワイヤーサイズを 0.038 inch へ減じてみました。あるとき実験的に、「(片側ごとに)もう1 個ループを増やしてみることにしよう。」と考えました。ヘルカル状のループが合わせて 4 個の試作品を圧縮してみて力の大きさを計測、こうして作られた装置は 600g の側方拡大力を発揮するので、正中口蓋縫合の拡大も理論上では十分可能です。
ところでほかの口蓋拡大装置では、すでに近心回転している上顎大臼歯の回転はそのまま残り、その後の捻転の修正は容易ではありません。これは以前から私が快く思っていなかったことでした。ところがこの装置を使えば大臼歯の遠心への回転は、口蓋縫合の拡大に並行して可能となります。捻転修正と鼻腔を含めた正中口蓋縫合の側方拡大が同時に行い得ることは、理にかなっています。さらに舌側に転位している上顎側切歯を前方に延長したラテラルアームにトモグラムで調べてみると、Wアプライアンスを使った患者では、口蓋の拡大像が確認されたので、これは単に歯を動かすだけではなく、それ以上の効果があることを、漠然とですが確信しました。使用したワイヤーは、直径およそ1mm(0.040 in.)の貴金属線です。引き続き正貌断層写真による確認作業をルーチンべースで行うことにしました。しかも、口蓋裂の患者以外でも同様の装置を用いて順当に口蓋が広がっていることを知りました。こうして、その可能性の広さを感じ取ったのです。
はじめの頃はバンドを外して調整し、再びバンドを合着するという作業を繰り返していましたが、大変に手間がかかりました。その対策として、 ワイヤーの弾性を向上させ、口腔内でも容易に調整ができるよう、装置のデザインを一部変更、バンドろう着部の後方にループ(Helix)を設けたのです。(金合金に最も物理特性が近いとされる)エルジロイワイヤーが開発されたのを機に、このワイヤーへ変更したのですが、力が過大であったため歯根の損傷を経験し、ワイヤーサイズを 0.038 inch へ減じてみました。あるとき実験的に、「(片側ごとに)もう1 個ループを増やしてみることにしよう。」と考えました。ヘルカル状のループが合わせて 4 個の試作品を圧縮してみて力の大きさを計測、こうして作られた装置は 600g の側方拡大力を発揮するので、正中口蓋縫合の拡大も理論上では十分可能です。
ところでほかの口蓋拡大装置では、すでに近心回転している上顎大臼歯の回転はそのまま残り、その後の捻転の修正は容易ではありません。これは以前から私が快く思っていなかったことでした。ところがこの装置を使えば大臼歯の遠心への回転は、口蓋縫合の拡大に並行して可能となります。捻転修正と鼻腔を含めた正中口蓋縫合の側方拡大が同時に行い得ることは、理にかなっています。さらに舌側に転位している上顎側切歯を前方に延長したラテラルアームによって唇側へ動かすことも、第一大臼歯の遠心回転に付随する形で進めることができます。このすばらしい装置は 私が最も活用してきたものです。以上が、Q/H の誕生の経緯です。
〔M.〕 Now, what kind of cases do you use a quad helix for today?
〔M.〕 現在は、どのような症例に Q/H をお使いになりますか?
〔R.〕 Oh God! It just seems like I use it a lot. Since that time, of course, Wilson with his technique... A lot of people like it. I don’t. I would still prefer to solder it. We have the removable quad helix now. It’s made in .036 steel. It doesn’t get quite the same results. But a lot of people like it, so they can use it. But, let’s start out with the high incidence of cross bites in the deciduous and mixed dentition. I will use it in literally all cross bites, and I’ll treat them bilaterally because usually there is a physiologic shift.
〔R.〕 いやいや、昔とほとんど変わりません。かつて多くの症例に 適用してきたのと同様です。爾来、ウィルソン氏は、既成のボディーワイヤー にバンドとフリクションロックをかける機構をそなえた Q/H を考案しまし た。多くの臨床家が好んで使っているようですが、私は従来の通りバンドにワイヤーをろう着しています。ウィルソン氏の Q/H では、ワイヤーサイズが 0.036 inch のスチール線が使われており、これでは同等の治療結果を得ることは難しいと思います。でも、多くの人々が好んで使っているのは 事実であり、あまり差し支えないと思います。まずは適応症例として比較的に頻度の高い、乳歯列や混合歯列期のクロスバイトに使うのがよろしいでしょう。私は、文字通りすべてのクロスバイトの症例に使い、両側性に拡大(左右均等に力をかける)します。というのも、(低年齢の場合)大抵の場合は、生理的な交叉咬合が生じているからです
〔M.〕 Right, I would agree with that.
〔M.〕 私もそう思います(低年齢児の機能的な交叉咬合に関して)。
〔R.〕 So we treat it and the mandible centers. In bilateral cross bites, we’ll treat for arch length deficiencies. In an arch where you come up at the age of eight, two incisors are in and the canines are in, but the laterals are displaced lingually and there is no space for them. You’ve got that problem.
We would use it in Class Ⅲ’s, and put reverse head gears on them. We would use it in Class Ⅱ’s, to also assist in the distalizing of a molar because one of the things that happens with it — and if you analyze the trajectories of the distribution of the forces, you’ll find how if you use it the way we do, the upper molar is going to move distally. So I have actually corrected, fully corrected, Class Ⅱ cases with the quad helix appliance. People don’t believe that.<
〔R.〕 そのようにして、下顎骨は正中に戻ります。両側性のクロスバイトでは、アーチレングスの獲得も目指します。例えば、8 歳の時に中切歯と犬歯が萠出していて、側切歯が舌側に転位している症例を考えてみましょう。側切歯の入るスペースは不十分です。放置すれば問題が起きてくるわけです。
Ⅲ級症例では、上顎骨前方牽引装置に Q/H を併用することもありましょう。また、Ⅱ級症例では上顎第一、第二大臼歯の遠心回転によって大臼歯を遠心移動させる補助として Q/H を使います。なぜなら、上顎第一大臼歯の舌側根は比較的長く、遠心回転によって頬側近遠心根は後方に動き、大臼歯そのものが遠心へ移動するからです。力の伝達経路を分析すれば、我々がやっているような方法をご理解頂けると思いますし、実際にも上顎大臼歯は遠心に動くのです。信じない臨床家もいるかもしれませんが、Ⅱ級の臼歯関係の是正が Q/H だけで達成できる場合も、症例の中にはあるのです。
 |
第14回 An Interview with Dr. Robert M. Ricketts 1987
2017.07.24
第14回:Arcial Growth 弓状成長の発見
An Interview with Dr. Robert M. Ricketts DDS, MS April 13, 1987
Copyright © 2015 University of Michigan School of Dentistry
Some rights reserved. Except where otherwise noted, this work is licensed under the following:
Attribution: Please attribute the work to the University of Michigan School of Dentistry and any individual author(s) cited. Not-for-profit: Use, display, and redistribute all or part of this work for non-profit and educational purposes only.
Share alike: Redistribute derivative works with the license listed here.
Visit the University of Michigan School of Dentistry’s website at http://www.dent.umich.edu/.
View the original interview at https://www.youtube.com/watch?v=lcBLmVOn3m0.
Interview conducted by James McNamara, DDS, MS, PhD. Interview transcribed by Yuri Shindo, MD.
Interview translated by Katsuyuki Shindo, DDS, PhD.
【 Arcial Growth 】
〔R.〕 By releasing the posterior support, taking the condyle away from the eminence, and letting the condyle grow vertically. That will take advantage of the arcial growth, and the chin will swing out under.
【 弓状成長の発見 】
〔R.〕 (バンドをかけた第二乳臼歯が僅かに挺出するので、)顎関節窩において下顎頭に対する応力の緩和がみられ、それに伴って下顎頭の垂直成長が促されると考えられます。(下顎骨は側面からみて円弧状に成長するため)下顎頭や下顎枝の垂直的な成長は、下顎骨のアーク状(螺旋状) の成長発揮に寄与します。螺旋に沿ってオトガイは押し出されるように成長するのです。
〔M.〕 Do you find that by doing expansion in the upper, you set up a template of the teeth so that, in fact, the mandible has to move a little bit more forward anyway?
〔M.〕上顎の側方拡大によって歯の配列も整うので、そこに向けて僅かに下顎が前方に成長するようになるのでしょうか?
〔R.〕 I think that you free it for movement, which I think in deep bites is restricted. I don’t think in terms of AP [anteroposterior] positioning anymore in the growth of the mandible, as much as I do vertical positioning. Not at the chin, but in the ramus. And I think it’s because - and I should talk to you about this because you look at as many joints as anybody I know - but my impression is that in the human, the bulk of the cartilage is on the anterior superior slope.
〔R.〕締めつけられたような過蓋咬合の場合、その状態を解放して下顎の自由度を高めることになると私は推察しています。(下顎が安定的に前方に発育促進された症例において、下顎頭や下顎枝全体が)垂直に発育する事実を目の当たりにして、下顎骨の成長を前後方向で考える従来の思考に対して、もう私は全く賛同致しかねています。「垂直」に成長するというのは、オトガイではなく下顎枝の領域のことです。それにつきましては… 是非とも付言しておかねばならないと思うのですが、どんな人の顎関節であれ、よく観察すればおわかりいただけると思いますが、下顎頭の上前方の軟骨における発育が下顎の発育に大きく影響を与えると私は感触しています。
〔M.〕 On the superior slope?
〔M.〕 上方湾曲部にある軟骨ですか?
〔R.〕 Yeah, and it grows superiorly. If you look at the back end of the condyle, a lot of times you’ve got resorption taking place.
〔R.〕そう、上方に発育します。下顎頭の後方を仔細に観察すると、 多くの場合、そこには(成長に伴って)吸収像が見られます。
〔M.〕 Well, I think Björk has shown that somebody that has a horizontal-growing mandible would be growing vertically at the condyle.
〔M.〕たぶんビョルク氏も、下顎が水平に発育する者においては、下顎頭の垂直的な発育が旺盛に起こっていることを報告していたと思います。
〔R.〕 That’s right.
〔R.〕 そうでしたね。
〔M.〕Which I must admit is a concept that I don’t think everybody totally understands.
〔M.〕この概念をすべての臨床者が完璧に理解しているとは、まだ言い難いですね。
〔R.〕 Well, that was one of the first things that I had to overcome also. In my 1952 paper, which was my prize-winning paper, we analyzed patients who underwent treatment in the previous five years. When you get backward growth of the condyle, the chin drops down. The cases in which the condyle was growing upward and forward, or the mandible was becoming more acute, were the patients in which the chins were growing forward.
Therefore, if you really wanted to change a patient’s pattern, it made sense that you wanted to get the vertical growth [of the ramus or the condyle] so that you could get the chin coming underneath the maxilla in Class Ⅱ’s. The opposite of that is the opening that takes place in Class Ⅲ’s while the chin is still growing forward. Those patients are developing the over closure.
〔R.〕 確かに、これは私にとっても第一に認識を改めなければならなかった事柄でした。私の 1952 年の受賞論文には、5 年の治療期間中に生じた下顎の成長変化を分析したものがあります。下顎頭が後方への発育した患者では、オトガイが下方に向かうかたちで成長してしまいました。ところが、下顎頭が上前方に発育した患者においては、下顎下縁平面の角度が浅くなって (Gonial angle が増加) 発育していき、そのような症例においては、オトガイが前方に発育していました。
したがいまして、患者のもつ成長パターンを本気で変えたいと望むのであれば、下顎枝や下顎頭の垂直的な成長を促すことを念頭に置かなければなりません。Ⅱ級患者ではこの成長変化によって、上顎に対して下顎骨が回り込むように前方へ発育していきます。一方、Ⅲ級症例では下顎のこの部分が発育すると、オトガイは前へ成長を続けるものですからオーバークロージャーが進むように観察されます。
 |
第13回 An Interview with Dr. Robert M. Ricketts 1987
2017.07.20
第13回 Orthopedic Change with Headgear ヘッドギヤーによる骨格変化
An Interview with Dr. Robert M. Ricketts DDS, MS April 13, 1987
Copyright © 2015 University of Michigan School of Dentistry
Some rights reserved. Except where otherwise noted, this work is licensed under the following:
Attribution: Please attribute the work to the University of Michigan School of Dentistry and any individual author(s) cited. Not-for-profit: Use, display, and redistribute all or part of this work for non-profit and educational purposes only.
Share alike: Redistribute derivative works with the license listed here.
Visit the University of Michigan School of Dentistry’s website at http://www.dent.umich.edu/.
View the original interview at https://www.youtube.com/watch?v=lcBLmVOn3m0.
Interview conducted by James McNamara, DDS, MS, PhD. Interview transcribed by Yuri Shindo, MD.
Interview translated by Katsuyuki Shindo, DDS, PhD.
【 Orthopedic Change with Headgear】
〔M.〕 For example?
【 ヘッドギヤーによる骨格変化 】
〔M.〕〔M.〕 具体的には?
〔R.〕・Simply where to put the tubes on the molars.
・How to construct the extra-oral headgear. Whether to use a bite plate with it or not. How much to use it. How much force to put on it.
・Whether or not to have the upper teeth banded at same time, which you shouldn’t do.
・How to adjust it on a daily basis.
・Which type of case that you select to use it on.
・What the possibilities and the probabilities of the growth pattern are, and so forth.
And that came out to be 22 mistakes that people had made in the past. If they don’t do head gear in the
right way, they’re going to get in trouble with it. And they did, didn’t they?
〔R.〕・ 左右の大臼歯 2 ヵ所にバンドを装着するだけで十分機能します。上顎歯列全体にワイヤーを・ 左右の大臼歯 2 ヵ所にバンドを装着するだけで十分機能します。上顎歯列全体にワイヤーを合、連続ワイヤーが正中口蓋縫合の拡大を阻害、上顎切歯は第二乳臼歯の遠心傾斜にともなって挺出、 上下切歯間の咬合干渉が Chin の後下方への回転を誘発)。
・H/G のデザインにも注意が必要です(※ インナーボウは、バンパー効果を発揮されるよう、インナーボウは歯列弓よりも円弧を大きくした形状にしなくてはならない)。
・バイトプレートの併用は禁忌です(※ 上顎第二乳臼歯が過剰挺出)。
・使用時間、使用期間についても配慮しなくてはなりません(※ 目安として 1 日 14 時間の装着、夜間は成長ホルモンの分泌で組織反応が高まっているので最適、日中は組織を休める)。
・力の大きさにも配慮を要します(※ 6 歳から 7 歳なら 350 g、8 歳前後 なら 500 gが目安)。
・上顎のほかの歯にバンド (ブラケット)を装着してはいけません。
・毎回の調整の方法(※ 僅かに大臼歯部を拡大し翼突板の外側を口蓋骨が回り込むようにインナーボウを拡大、かつ大臼歯を徐々に遠心回転させる)や、一応の改善をみるまでは毎晩患者に装着してもらうことも大事です。
・症例の選択を誤ってはいけません(※ High convexty case で、かつ比較的筋肉と骨格がしっかり、また扁桃や指しゃぶりの問題があればこれも事前に解消しておく)。
・成長の可能性と成功の確率性を客観的かつ冷静に吟味する...、などです。
これらに照らしてみたら、22項目の誤りを臨床家が犯していたことが判明しました。もしも H/G の臨床技術そのものに問題がありますと、矯正歯科医は痛い思いをせざるを得ません。実際、その通りのことが起きましたね。
〔M.〕 Yeah.
〔M.〕 そうでした。
〔R.〕 People made such gross errors with it. In my experience, with the proper use of the headgear, I can stimulate the mandible to grow.
〔R.〕 人々の誤用は甚しいものでした。また、私の経験では、適切に H/G を用いた場合、下顎骨の成長は刺激されると考えられます(※ 大きく目に見える形ではなく微かに、着実に発揮)。
〔M.〕 How do you do that?
〔M.〕 その機序についてご説明頂けますか?
写真は、劇作家の松居松葉(まつい しょうよう)の『金賣吉次(かねうりきちじ、明治9年刊)』の挿絵。明治三年生れの松葉は、上京し2年ほど、日本近代歯科医学の父と呼ばれるWilliam Clark Eastlake(1834-1887)の家に寄宿、イーストレーキーが妻ナオミとともに神田の地に起こした英語学校(後の国民英学校)に学ぶ傍ら彼の翻訳の手伝いもした。
 |
 |
第12回 An Interview with Dr. Robert M. Ricketts 1987
2017.07.04
第12回:Early Treatment 早期治療の追求
An Interview with Dr. Robert M. Ricketts DDS, MS April 13, 1987
Copyright © 2015 University of Michigan School of Dentistry
Some rights reserved. Except where otherwise noted, this work is licensed under the following:
Attribution: Please attribute the work to the University of Michigan School of Dentistry and any individual author(s) cited. Not-for-profit: Use, display, and redistribute all or part of this work for non-profit and educational purposes only.
Share alike: Redistribute derivative works with the license listed here.
Visit the University of Michigan School of Dentistry’s website at http://www.dent.umich.edu/.
View the original interview at https://www.youtube.com/watch?v=lcBLmVOn3m0.
Interview conducted by James McNamara, DDS, MS, PhD. Interview transcribed by Yuri Shindo, MD.
Interview translated by Katsuyuki Shindo, DDS, PhD.
【 Early Treatment 】
〔M.〕 Now when you say“early treatment”, what do you mean?
【 早期治療の追求 】
〔M.〕 あなたの仰る「早期治療」を、具体的にお聞かせ下さい。
〔R.〕 I’m talking about even in the deciduous dentition. That to me is“early treatment”. It’s not early until it gets in the deciduous dentition. We can look at your own daughter’s casts there if you don’t believe in early intervention.
〔R.〕 乳歯列期の患者を対象とした処置も含みます。私にとっての早期治療とは、子どもたちが低年齢の時期における治療を指します。乳歯列期に達していない場合は、「早期治療」とは呼びません。あそこにあったお嬢様の歯列模型を見れば、早期に行う介入処置の大切さがご納得頂けるでしょう。
〔M.〕 Oh, I know. Sure.
〔M.〕 分かります。確かにそうですね。
〔R.〕 I mean [her maxilla] has been widened that far, and she doesn’t look like she’s expanded. In fact, she looks like she needs more to me. And she does.
But you’re not going to get that if you wait until the patient is completely grown. These possibilities do not exist, particularly with females at puberty. They’re already over the hump. And you are not going to get some of these things done. You can still treat them, but don’t treat them in the same way. So this took me into early treatment - what I call the“prevention stage”. Preventing the malocclusion from involving permanent teeth by treating deciduous dentition. That’s what we mean by “ prevention”.
“Interceptive”, then, is intercepting the transition from the deciduous to the mixed dentition, and from the mixed dentition to the permanent dentition. That whole broad gamut is“interceptive orthodontics”. Then“corrective”. And finally, when all effective growth has ceased, we then go into what we cal“l rehabilitate orthodontics”and “rehabilitate techniques.”
〔R.〕彼女は上顎の拡大処置を受けたのでしょうが、時期が遅すぎたようなので、私からみるとまだ十分とは思えません。もう少し拡大なさってはいかがでしょうか。実際彼女にとって必要です。
仮に成長が完了してしまうと同様の結果を得ることはできません。改善の可能性は失われてしまい、とりわけ女性では思春期に差し掛かると、この傾向はさらに顕著になります。成長の旺盛な時期はすでに過ぎ去っていますから、手持ちの札は限られてしまい、同様の結果を得ることは出来なくなります。勿論、治療を継続することはできますが、同じ方法を採用することは無理です。これが私を早期治療に駆り立てる原動力になりました... すなわち「予防段階」と私が呼ぶところの処置です。乳歯列期に治療を行い、不正咬合が永久歯に波及するのを阻止するわけです。目標は、永久歯の健全な萠出、すなわち不正咬合の進展を予防することです。
次の段階が、「インターセプティブ」、つまり不正咬合が悪化していくのを防ぐ段階です。乳歯列から混合歯列、あるいは混合歯列から永久歯列へ、不正咬合が増悪していくのを阻止するわけです。この範疇の処置のすべてがインターセプティブな治療となります。成長が終了してしまった後の治療は「コレクティブ」、すなわち不正咬合に対して修正をかける段階となります。それを過ぎて、何らかの病的な状態に陥ってしまった場合は、「リハビリ的な矯正歯科治療」になります。
〔M.〕 Now, when you talk about interceptive treatment, what specific treatment modalities are you dealing with?
〔M.〕 インターセプティブということですが、その中であなたが扱っていらっしゃる独自の治療様式(Modalities)をお聞かせ下さい。
〔R.〕 First of all, you have to think of a treatment as primary, not finishing, technique. You’re not going to finish the case at this time, so you’re talking about intercepting the development of the malocclusion - altering skeletally, changing the environment, setting the stage for normal development of the permanent side teeth or the incisors if it’s a deciduous case.
So this is what I’m talking about now. Any modality that will do that. So if a dysplasia is in an upper arch, you’ll have extra-oral traction. As you know, I have 28 mistakes that people made with an extra-oral traction. Twenty-eight of them.
〔R.〕 まず踏まえておくべきことは、インターセプティブという治療概念が初期段階の処置を指すことです。最終的な仕上げを目指すものではありません。この段階においてすべての問題を解決することは現実的ではないため、不正咬合の増悪を阻止する概念となりましょう。具体的には、骨格を是正し、口腔内環境を正常な状態へ整え、側方永久歯列群の正常な発育を促し、乳歯列であれば永久切歯の正常な萠出の基盤を整える、ということです。
ポイントを押さえておくのが肝要です。あくまでも治療様式の目的はここに集約します。仮に上顎骨に形態上の問題があれば、口腔外牽引装置の選択を考慮しなければなりません。ご存じの通り、口腔外牽引装置(サービカルトラクション等)を例にとると、人々の用法に 28 項目におよぶ誤りがあることを以前指摘しました。28 項目もですよ。
 |
第11回 An Interview with Dr. Robert M. Ricketts 1987
2017.04.22
第11回: Innovation and Invention あふれる才気
第11章は、論語の君子有九思の「疑思問」に相当するかも知れません。
ここではRicketts R. M.が意識無意識に抱きつづけてきた、結果検証主義の壁を打ち破る『自在な演繹思考」とみてみましょう。
ところで昨今は、先人の示した結果を覚えるのに手一杯、そこへ学会のガイドラインが次々に提示される‥‥そんなせわしくも、がんじがらめ観がありますが、「疑思問」は、「常識に潜む見当ちがい」を察知し、患者さんへ個別の良質な医療を提供するひとつの鍵だと思っています。
「なにかヘンだな?」を大切に
VTO作成を通して、「なにか自分が未知の出来事が生体に起こっているはずだ」と問うことで、つぎに、Orthopedicな治療変化を実証。さらにはそれが早期治療へとRicketts R. M.を駆り立てた原動力になっていたことが物語調に語られています。
中顔面の一連の骨は、頭蓋基底から吊される構造で、咬合の応力負荷に耐える構造を除けばとても軽い‥‥鼻甲介や篩骨を掌にのせると、お麩よりも軽くてビックリ。
それほど生体は、「Maximum benefit with the least amount of energy」を地で行く。骨だけでも上顎骨・口蓋骨・頬骨・鋤骨・篩骨・涙骨・下鼻甲介・鼻骨。成長中にはそれぞれが「スゴ技」を発揮します、例えば口蓋骨は蝶形骨翼状突起との間で縦方向の成長を調整し、上顎骨との間で横方向の整合性を高め、嚥下や発語に絶妙な筋肉のフックを提供する‥‥などなど。
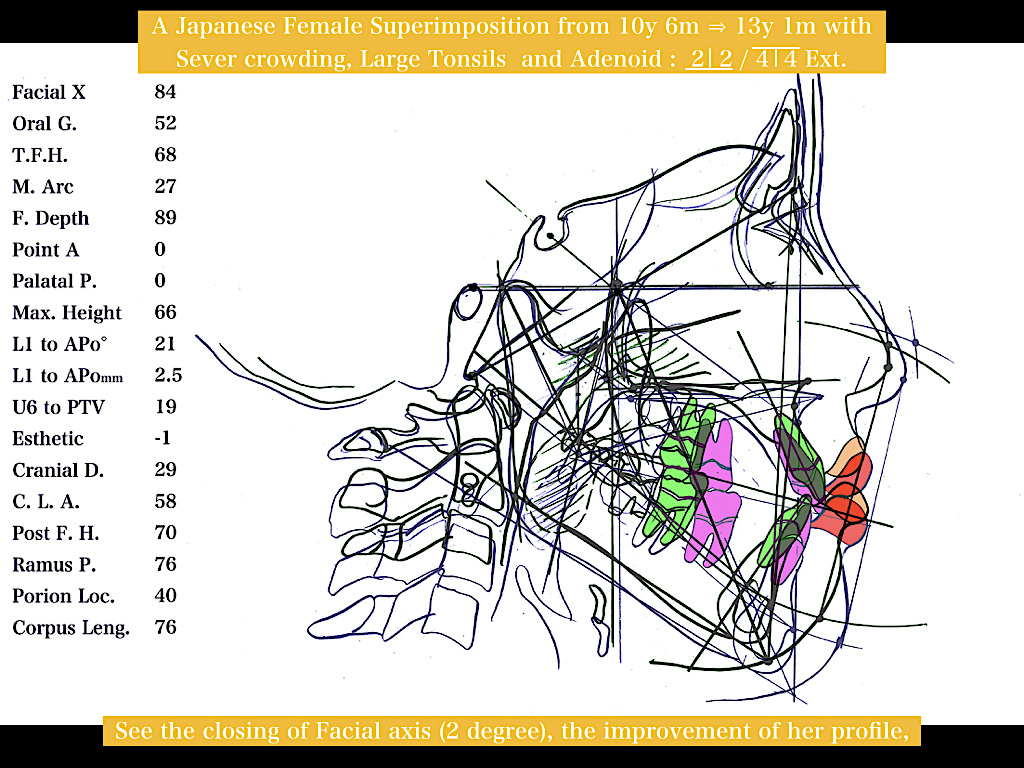
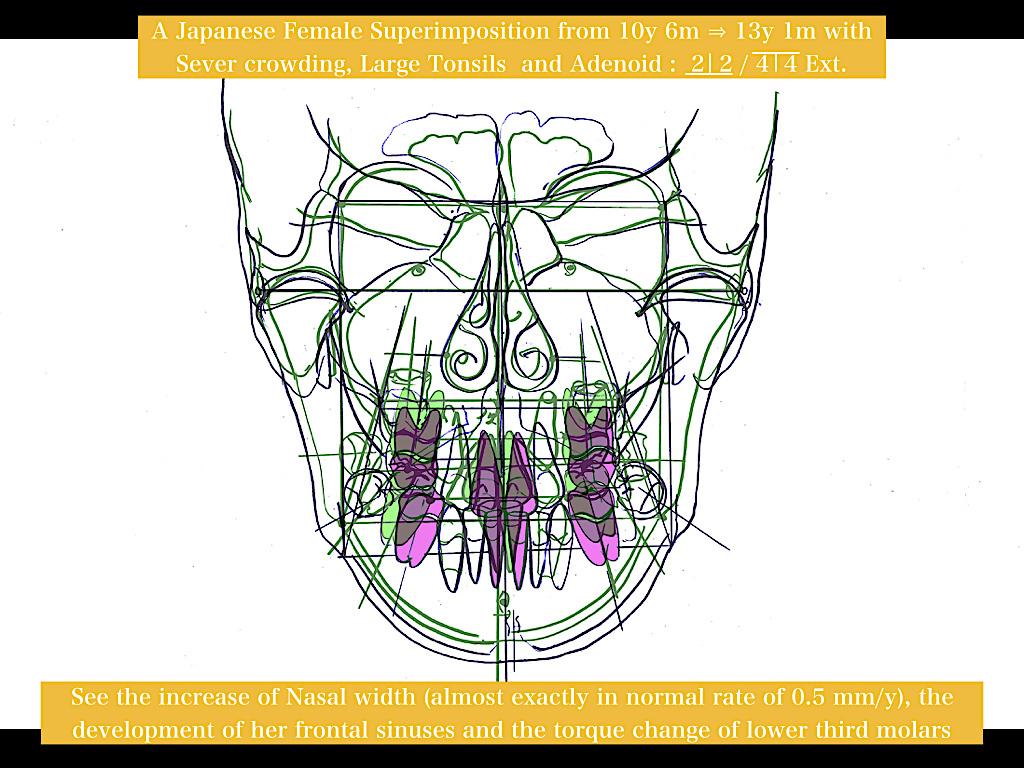
Orthopedicな変化は、7,8歳までに行われる早期の矯正歯科治療において、Ⅰ級、Ⅱ級、Ⅲ級の大方の症例において、側貌や正貌セファログラムに確認することが出来ますが、鼻腔の形成にもこれらが参与することから、鼻呼吸の生理化にもOrthopedicな変化が貢献することが、多くの研究者から報告されています。
【 Innovation and Invention 】
〔M.〕 What do you think are your - let’s take those pillars, and let’s look at the treatment aspect of things that you do today or 20 years ago that you were taught you“couldn’t”do. Now clearly, utility arches are one of the things that you would be talking about with regard to the intrusion of the teeth. Including that, what other specific treatment aspects -
【 あふれる才気 】
〔M.〕 そのときのあなたの... 思想の後ろ盾を成した技術、つまり今日実践していらっしゃる臨床技法、あるいは教条主義に警鐘を鳴らしていらした 20 年前に考案していらした治療手技もみてみたいと思います。たとえば誰もが知る通り、歯の圧下移動に関してあなたは各種のユーティリティーアーチを開発され、これによって歯の圧下移動が不可能ではないことを人々に示されました。これを含めて、どのような臨床が生まれたのでしょう?
〔R.〕 Well, let’s start out maybe with how I discovered them in the first place. I started setting up cases in 1950 for surgery and for orthodontics.
The first surgical VTO [visual treatment objective] I did was in 1950. So the same theory can be applied to the surgical cases. The only difference now was putting growth, teeth, and physiologic anticipations into consideration once we knew that this was the likely result of the therapy. We can take that right into our removable appliances today because now, with the differences in behaviors, we can anticipate those kinds of things. So to say that all treatment is going to give the same result, and that the teeth don’t know which appliance is on is absolute folly. So let’s go back, then, with maybe the real arresting changes that we made and how we came to them. And I suppose the first one would deal with the fact that we begin to see things taking place orthopedically. And I think that probably set me off more than anything.
〔R.〕 発見の端緒に遡って説明致しましょう... そこが肝要ですから。外科矯正症例と通常の矯正歯科症例の、双方の治療目標を(セファロトレース図をもとに)製作したのが1950 年でした。
今日でいう「VTO(目で見る治療計画)」を作った第一号患者は外科症例でした。成長は考慮しなくても済む症例とはいえ、顎や歯列の移動にともなう軟組織の変化については、成長患者と概ね同じ予測が当てはまります。一方、小児の矯正歯科症例では、成長、歯列の位置、生理学的な変化を、治療経験に照らして予想値として組み入れることによって予測します。種々の可撤式矯正装置を用いた治療変化についても、装置ごとに生体の反応がどう異なるかが分かってきましたので、予測が可能となりました。ですから「どんな治療法を採用したところで結果は同じ」、「治療結果からは装置の種類を推察不能」... という従来の考え方が全くの誤りであることも明らかになりました。
そこで、我々の革新事業の中で、たぶん最も注目すべき変革と、その契機について振り返ってみましょう。まず発端は、歯列だけではなく、顔に対して orthopedic な変化が実際に起きていることへ気がついたことです。何よりもまして、この発見が私を衝き動かしたと思われます。
〔M.〕 Are you talking mostly extra-oral traction here?
〔M.〕 おもに、口腔外牽引装置を使ったときの変化でしょうか?
〔R.〕 Yeah. One of the other things that I had to say was the rest position of the mandible. You know, we used to say that the rest position was unchangeable and all that. That would go with the 24 things about the rest position, dealing with the joint, and a few other things. So there were a lot of these little things that were wrapped up in there. That you always had to have a CO [centric occlusion] and CR [centric relation] together and all that. Terminal hinge, really, at that time. So I kind of put those things in there too.
And I’d set up these cases on the basis of my experience with treated cases at the university. And I found it didn’t work. I was making mistakes. My treatment was beating the prediction all over the place. I’m not talking about a millimeter, I’m talking about a quarter of an inch. So this was no longer anything. Of course, I was told that the maxilla was immutable, that you couldn’t do this. I was told that these things wouldn’t take place.
So having discovered that, having also opposed the idea of constant physiologic rest position, that you couldn’t intrude teeth, that you couldn’t move upper molar back - it was unthinkable that you could move the lower molar back. I suppose that then was the basis for the controversies that started. So that’s what started. Now, what was your question again?
〔R.〕 ええ。もう一つは、下顎安静位にまつわる従来の認識の誤りに気がついたことでしょう。ご存じの通り、かつては下顎安静位というものは不変であると信じられていました。顎関節やほかの二、三の関連事項を含めれば、下顎安静位に関する修正だけでも 24 項目にのぼりました。重複する発見をまとめる形で分かりやすく論著に提示しました。当時は、「最終蝶板位」や「中心咬合位」あるいは「中心位」という概念がやかましく叫ばれていた時代です。これらの混乱も整理して追加しました。
(ここから成長予測法の話題に入ってきますが...)医局在籍中の自分の臨床経験に基づき、これらの症例について成長を予測してみることにしました。ところがどうもうまく予測出来ないのです。どこかが誤っていることは明らかでした。治療結果と成長予測は至るところで整合性を欠いている有り様でした。今話しているのは 1mm 程度の問題ではなく、1/4 inch にもおよぶ誤差です。したがって何か自分がまだ知らない実質的な変化が起きているに違いない、そう考えました。勿論私は、「治療によって上顎の成長を変えることは不可能」と教育を受けてきた世代です。
こうした過程を経て、口腔外牽引装置を適用すれば、上顎の成長を変えることができることを発見しました。そのほか、下顎安静位の定常性の概念、歯牙の圧下移動は不可能、上顎大臼歯は遠心移動できない、ましてや下顎大臼歯の遠心移動は到底無理に決まっている、といった「当時の常識」に対して反駁に足る確証を蓄積していきました。正しい概念を広く示す我々の活動は、このようにして始まったのです。ところで、先ほどのご質問から外れるといけないので、主旨をもう一度お願いします。
〔M.〕 Well, I was trying to look at the specific treatment modalities that you have instituted.
〔M.〕 (やおら気圧されたあと...)あなたが独自に開発なさった治療システムについてお聞きしようと思いました。
〔R.〕 Okay. Well, we came out with the fact that you needed to treat patients at a young age. And, in my opinion, if you get the patients at these ages, by this treatment and other modalities, you’ve saved them from surgery because there’s a tremendous surgical movement in the country today. I don’t know whether you know this - well, I’m sure you do - the depth of it that’s out there. There’s almost as many surgeons being trained today as there are orthodontists. And who are they going to operate on? They’re going to operate on orthodontic failures. That’s what’s taking place.
〔R.〕 分かりました。小児を対象とする早期治療の必要性が強く認識されるようになって来ましたので、その重要性さを我々は提言しました。骨格的な是正を行い得るような低年齢の子供たちを、我々の開発した方法、我々の推奨する装置の取り扱い方で処置することができれば、個人的な見解としては、子どもらが外科矯正処置へ移行するのを大幅に回避できると思われます。現在、米国においては狂気の沙汰としか思えない勢いで、「外科処置で解決を図ればよかろう」との思想が蔓延しています。問題の深刻さについてはよく承知していらっしゃると思います。矯正歯科医とほぼ同数の口腔外科医が、顔面骨格の外科的是正処置のトレーニングを受けています。外科治療は誰を対象として行われているかご存じですか? 早期治療の有用性を見逃して失敗した矯正歯科医の後始末をしているような構図です。これが現実なのです。
 |
 |
第10回An Interview with Dr. Robert M. Ricketts DDS, MS April 13, 1987
2017.03.17
第10回: The Challenge 教義への挑戦
山帰りの温泉で、西丸震哉さんの『山小舎を造ろうヨ』 — 少し人生を考え直したい人に!(中公文庫)を読んで思わずうなずいてしまった。
「都会に住んでいて、一生その中から出ないでいても平気でいられる人は読まない方がいい。私の好きな人で、文化庁の長官だかになったひとだが、彼は『山? 自然? 緑? 興味ないねえ。ボクは六本木あたりのバーに入りびたっているのが幸せだ』とのたもうた。」
「他人と同じ事をやっていないと安心出来ないという恐怖心は、じつは日本が二千三百年の間、水田稲作社会を続けてきたために出来上がった考え方だ。」というのが西丸さんの動物的感触、というより西丸さん御自身はきわめて野生動物に近接した人だったから、明晰な頭脳を兼ね備えた一生物の「観察」と私はにらんでいる。
それはともかく、時折、西丸さんの著作に力を得て、かすかに残った野性感覚を頼りに世間を見渡してみていると、西丸さんとRicketts R. M.さんが面白く重なってくる。
すると、点数上の優劣と無関係な、「思い込みの強さと、飲み込みのわるさ」が蔓延っていることにあらためて驚かされる‥‥アタマの構造そのものが、自分を眩ませて済むように、組まれているからだそうであるが、振り返れば勿論私も例外ではない(笑)。
【 The Challenge 】
〔M.〕 Now in 1968, you published a paper on - I guess to put it simplistically - all of those things you were taught you couldn’t do that you can do. How about going through some of those for me?
【 教義への挑戦 】
〔M.〕 ところで、1968 年に興味深い論文をあなたは書いていらっしゃいます。生物学的には可能性が望めるにも関わらず「不可能」であると臨床者が教え込まれて来た内容についてです。当時の矯正歯科医が思い描いていた誤った「常識」... これについてもお話を頂けますか?
〔R.〕 Okay. Well let me give you a little bit of background for that paper in the first place. In 1967, I took my family and went to Europe. My wife, at that time, and two daughters preceded me, and they spent three months in Europe. I rented the home out and had my son in a camp. So I lived in Riviera Country Club, and rented our home out which wasn’t too bad. And I was supposed to go over there. I went for two weeks on vacation, and then I started circling and lecturing.
I had gone to Scandinavia, and I put on a course in Spain and I think in France. Then I was to end up that lecture with an address in London ― just an evening meeting in London. And I wondered what I was going to say in London when I got there because I had already experienced several conflicts with people in England who were really entrenched in the Doctrine of Limitations. So much so that many people wouldn’t try to treat the lower arch, as you know.
〔R.〕 了解しました。まず初めに、なぜこのような論文をまとめるに至ったか、その背景についてお話いたしましょう。1967 年、私は家族とともにヨーロッパへ出かけました。妻と娘の 2 人は先に出発し、彼女たちはそこで 3 ヶ月間を過ごしました。息子はその間コロラド州の夏キャンプに参加、私はリビエラカントリークラブにある中々快適な家で過ごし、ゴルフを楽しむ一方で、マドリッド、コペンハーゲン、ストックホルム、パリで開催するコースの準備に多忙な毎日を過ごしていました。そして 2 週 間の休暇後、ヨーロッパ各地を講演して回りました。
スカンジナビア半島の国々、スペイン、たしかフランスでも、そしてロンドンで講習と講演の活動を終えました。この頃すでに私は、英国の人々と臨床に関する意見の折り合いがつかず、彼らが「教条的制約(Doctrine of Limitations)」を頑なに信じ込んでいる実情を知るにおよんで、ロンドンではいったい何をどう話せばよいものやら思案に暮れていました。多くの禁止事項が、あたかも教義のように人々の頭を染め上げてしまっている有り様には参りました。一例を挙げるなら、ご存じの通り彼らの多くは、下顎の歯列には一切手をつけようとすらしませんでした。
〔M.〕 The Doctrine of Limitations coming from Nance’s article?
〔M.〕 「教条的制約」... 引用はナンス氏の論著でしょうか?
〔R.〕 Well, they were using that as a vehicle, but somehow or another with the scheme that they had there, they were -
〔R.〕イギリスの矯正歯科医はこの言葉を、みずからの正当性を弁明する「媒体」のごとくに扱っていましたが、当時の社会制度に由来する制約も加わっていたわけです。彼らは...
〔M.〕 What do you mean by“scheme”?
〔M.〕 あなたが仰る社会制度とは、英国の医療保険制度のことでしょうか?
〔R.〕 The social scheme.
〔R.〕 公的保険制度です。
〔M.〕 Oh, okay. You mean the National Health Service?
〔M.〕 分かりました。政府が運営する健康保険制度のことですね。
〔R.〕 The National Health Service. They call it the“scheme”. And I remember, at that visit - or maybe before, I don’t know - I knew Jack Tulley very well, was entertained in his home and so forth. And I went in and saw the cases that he had. So I went there with him, and I saw the cases. We went to have tea. We were there for about an hour and a half, and it was time for tea in London!
So we went back and he said“, Well, what do you think?”So I said“, What do you mean what do I think?”“What do you think of our treatment?”And of course I was in shock. I said“, Well...”I hated to say it, but in my mind I thought there were some cases that didn’t look much better than when they started. And I said“, Well, in my opinion, you’re just ready now. You’ve done your primary treatment, now you’re ready to finish the case.”And that was as much as they could offer to the patient.
The irony to me was that they had used all of the knowledge that was in orthodontics out there to justify that that approach was as good as anything else they could do. Well, of course, this I opposed. So I knew that they were in this whole philosophy of“you couldn’t do this, you couldn’t do that”.
So I came back from the lecture in London. While on my trip, I had gone through the Greek islands, and I had visited Ephesus. And I had seen all of the crumbling pillars, and I had stood in the amphitheater where [Apostle] Paul addressed the Ephesians. And it was one of the greatest experiences in my life, to sit there - or stand there - in his place, and realize that this was all history and that this abandoned town was really still there as it was in the beginning. So when I got there at London, I labeled my lecture“The Crumbling Pillars of Orthodontics”. Have you ever heard it?
〔R .〕 英国の健康保険制度です。彼らは「公的制度」と呼んでいました。それ以前の出来事かどうか忘れましたが、私は知人、ジャック・トリー氏の自宅に招かれ、症例のいくつかを閲覧したあと、意見を求められました。午後の紅茶を飲みに出かけましたが、1 時間半ものんびり過ごすロンドンの風習には驚きました。彼の自宅に戻り、「いかが思われましたか?」と尋ねられました。「何についての感想ですか?」、「我々の治療方法についてです。」こんなやりとりが交わされましたが、正直なところ、見せてもらった症例は私にとって失望を禁じ得ないものばかりでした。失礼に当たるので口には出しませんでしたが、症例のいくつかは治療前より少しも良くなっていなかったので、「歯を並べる準備としての基本治療は終わっているようなので、仕上げの処置に進まれてはいかがでしょう。」と答えるのが精一杯でした。親身に患者対応するのであれば、それが筋であると思ったからです。
皮肉なことに、彼らは折角の知識を、治療の正当性を証明するために使い回しているのではないかと残念に思われた次第です。勿論、私からすればこれは事実を歪曲した解釈に過ぎません。「あれもこれも不可能」 ... みな語るに落ちる思い込みに過ぎないと私は内心で感じていましたから ...。
私たち家族は、文明の発祥の地であるギリシャを休暇の折りに訪ねてみようと計画していたので、これを機に私は長男とアテネに飛んで先にヨーロッパにいた妻と娘 2 人、そして娘の友人とアテネで合流しました。一行 6 人でギリシャの島々を訪ね歩き、エピソスへ足を踏み入れました。遺跡の柱が崩れ落ちているのを目の当たりにして、詩人ポールがエピソス人に使徒の書簡を歌ったと伝わる円形劇場に座り込んでは立ち尽くす自分に気がつきました... 心が大きく揺さぶられる瞬間... まさしく彼がいた場所で、「すべてが歴史の一コマ。廃墟と化した街は昔と変わらず今なおここに...。」この言葉を胸に刻んだのです。ヨーロッパ講演の最終訪問地ロンドンに出かけた私は、自分の演題を「矯正歯科における瓦解した柱」と名付けました。あなたもご存じですか?
〔M.〕 Yeah I knew that. I’ve heard you say that but I didn’t know the background.
〔M.〕 あなたがそう仰っていたことは聞いておりました。でも、背景までは知りませんでした。
〔R.〕 So that’s when I started putting this list of things together that I could no longer believe. That’s what started it. That was in the summer, and that fall then, I addressed the Angle Society in New Orleans. They had the national meeting, and I was asked to be on the program. So I enlarged that talk and I labeled it at that time“Public and Professional Problems in Orthodontics”because at that time, we were beginning to see that there were a lot of problems in orthodontics with general practitioners. And it was my feeling that one of the things that we should do was become stronger and unite in our own knowledge, in our own philosophy, because there were a lot of different people out there. The Crozat craze was taking over at that time, and general practitioners were just now starting to experiment in orthodontics. And this was 20 years ago.
So I said“, Well, we should get our act together.”This was a plea to get our act together. And so I started it out by listing all of these different things that I had been taught that I could no longer trust and that I couldn’t believe. I could no longer use this as the bedrock of truth that I was told that it was. And it started out with one thing, the constancy of the pattern.
〔R.〕 これを契機に、誤認やら妄想の類として棄却すべき事項を洗いざらいリストに挙げていきました。そして、その夏の終わりから秋にかけてニューオリンズで開催された米国アングル学会において、演者の一人としてこのことを報告しました。ただし演題の内容は少し広げ、「矯正歯科における公衆と専門医を蝕む問題」と題し、会場の人々に提言したのです。というのも当時、すでに一般歯科医が矯正歯科治療へ経済進出してきた結果、これが数多くの臨床上の問題を引き起こす実態が浮かび上がってきたからです。我々専門医は一致団結して、学派や派閥を超え、互いの臨床知見と哲学を統合することで、この社会情勢に適切に対処すべきである、そう私は考えたのです。クローザット装置がやたら流行していた時代で、一般歯科医は歯を動かす手始めに、この装置を使っていました。もう 20 年も前の出来事です。
そこでわたしは「互いの協力の許、解決に立ち向かおう」と請願したわけです。かつては専門常識であっても、誤りは誤りとして直ちに棄却すべきであると確証されるに至った内容、すなわち臨床の礎石としては相応しくない迷信蒙昧のいっさいを払拭すべく、それらをリストに挙げていったのです。はじめに私が指摘したのが「パターンの定常性」です。
〔M.〕 You mean the Brodie type?
〔M.〕ブローディ式のことですか?
〔R.〕 Yeah, the Brodie type constancy of the pattern. Think about it for a minute. If you can’t do anything skeletally, then what are you left with? You’re left adjusting the teeth to the skeleton. That’s to get teeth adjusted. That was one of the things that added to this whole idea of extraction, that you just shift the teeth around within the c o n fi n e s o f w h a t y o u ’ r e w o r k i n g w i t h “. Y o u c a n ’ t i n t r u d e t e e t h . ”“ Y o u can’t move an upper molar distally.”
〔R.〕 ええ、彼の述べた「パターンの定常性」のことです。一寸考えてみて下さい。もしも骨格的な変更が不可能であるとの前提に立てば、残された治療手段はずいぶんと制約されたものになります。不調和を来した顎骨の上で歯を動かすしか手はありません。ひたすら歯を動かす処置に没頭するだけ、となりましょう。しかも成長中の可変要素を利用できないとなれば、(小臼歯)抜歯の比率が高くなるのは当然の成り行きです。歯を動かすだけの処置の限界に、矯正歯科専門医がみずからを追い詰めてしまうことになるわけです。しかも「歯の圧下移動は無理」、「上顎大臼歯の遠心移動は不可能」とまで決め込む始末でした。
〔M.〕 I can remember having discussions in my own orthodontic program in which our faculty in 1966 were arguing that exact point.
〔M.〕 1966 年の私自身の大学教職員の矯正歯科学会でも、論議の的はまさしくそこにありました。
〔R.〕 That’s right, that’s right“. You dare not expand.”“All expansions will move the lower incisors forward.”“You dare never move the lower incisors forward.”“You can’t change the oral environment.”You see? It went on to 24 things, and it later grew to 30 things that you“couldn’t”do.
〔R.〕 その通りです。「歯列弓の側方拡大はご法度」、「そもそも拡大とは下顎前歯を前に倒すに過ぎない」、「下顎前歯は前に動かすべからず」、「口腔内環境の変更は無理」... こんな馬鹿げたことがありますでしょうか? 24 項目もリストに挙がりましたが、後日「不可能」と決めつけられていた事項を加え、計 30 項目にも及びました。
〔M.〕 Can you remember any other ones?
〔M.〕 「教条的制約」で、ほかに思い浮かぶことはありますか?
〔R.〕 Well, the main ones turned out to be ― we can condense them down about seven of them:
・“You couldn’t use the intermaxillary elastics without moving the lower arch forward.”There was no such thing as cortical anchorage. ・“You couldn’t use muscle anchorage.”You treated to the muscle rather than using the muscle.
・“You couldn’t widen the palate.”You couldn’t do anything orthopedic [by using extra-oral traction].
・“You couldn’t predict growth.”
・“You may rotate the mandible open but it’s always going to recover.”
How many is that?
〔R.〕 まとめれば、概ね 7 項目に分類できます。 ・下顎歯列を後ろに保ったまま、II級顎間ゴムを使う技術などあり得ない
(※ 皮質骨の固定源への利用や Quadratis inferiolis labii の活用への配慮がなかった)。
・筋肉をアンカレッジに利用することは不可能(※ 特定の筋肉の特性を活用した処置を検討するのではなく、異常な筋肉に対して無理矢理、歯を動かしていた)。
・正中口蓋縫合の拡大は絵空事(※ あらゆる orthopedic な処置は不能であり、ましてや口腔外牽引装置を用いた顔面骨格の是正など有り得ないと信じられていた)。
・顔の成長予測を試みるなんて野暮の骨頂。 ・治療中に下顎骨が後下方へ回転することがあっても必ず元に戻る(※ 医原性の損傷は元に戻らないにもかかわらず...)。
思いつくままいくつか挙げてみましたが、いくつありましたか?
〔M.〕 It’s a lot.
〔M.〕 きりがありませんね。
〔R.〕 You begin to see what I’m talking about. Go through the list and add the few more we added years later. So we had these really down to about seven things“. You couldn’t do things orthopedically”“; you couldn’t intrude teeth”“; you couldn’t move the molar back”“, you couldn’t change the oral environment”“; you couldn’t predict growth”“; you couldn’t call your shots”“; you couldn’t predict anchorage”. All of these kinds of things.
So on the basis of that, I made recommendations to the profession, which I’ll be talking about tonight a little bit. And that was in 1968 when that was published. So it took a year from 1967 to 1968 And I remember working with Authur B. Lewis at that time on that paper, and he said that it was too much for one paper. So we broke it into two parts, so it’s actually a two-part paper - 1968 and 1969, or maybe all in 1968, I forget.
〔R.〕 意図するところをお分かり頂けたでしょうか。このような「教条的制約」のリストへ、後年、さらに二、三を付け加えることになりました。いずれにせよ、大別すると 7 項目に及びました。「orthopedic な変化をもたらすことは不可能」、「歯の圧下移動は無理」、「大臼歯の遠心移動は不可能」、「口腔環境内は変えられない」、「成長は予測不能」、「矯正歯科医が治 療を采配することなど無理(なるようにしかならない)」、「アンカレッジを(事前に)見積もることなど出来るわけがない」...。この類いの決めつけが矯正歯科界を暗雲のごとくに覆っていたのです。
そのようなわけで、これらの検証結果を踏まえて、専門医たちに治療上の新たな指針を提示し、改革を促しました。今夜そのことについても 触れてみましょう。1968 年には、これらが論説として出版されました。1967 年~ 1968 年の一年間にわたり、アサー・ルイース氏とともに論文を書き上げていきましたが、1 編にまとめるには多すぎるから 2 編に分けて公表した方がよいのでは、との彼の提案に従い、結局 2 編に分けて掲載しました。1968 年と 1969 年でしたか、いや 1968 年のことであったかもしれません。
 |
 |
第9回 An Interview with Dr. Robert M. Ricketts DDS, MS1987
2017.01.18
第9回:Clinical Research 臨床研究
Copyright © 2015 University of Michigan School of Dentistry
Some rights reserved. Except where otherwise noted, this work is licensed under the following:
Attribution: Please attribute the work to the University of Michigan School of Dentistry and any individual author(s) cited. Not-for-profit: Use, display, and redistribute all or part of this work for non-profit and educational purposes only.
Share alike: Redistribute derivative works with the license listed here.
Visit the University of Michigan School of Dentistry’s website at http://www.dent.umich.edu/.
View the original interview at https://www.youtube.com/watch?v=lcBLmVOn3m0.
Interview conducted by James McNamara, DDS, MS, PhD. Interview transcribed by Yuri Shindo, MD.
Interview translated by Katsuyuki Shindo, DDS, PhD.
An Interview with Dr. Robert M. Ricketts DDS, MS April 13, 1987
Vistas in Orthodontics (1962刊、99-130)の第4章を Ricketts R. M.が執筆しています。標題は『Cephalometrics — Clinical research in Orthodontics』。参考文献26編のじつに23編を彼自身の論文が占め、まさしく当時の研究の集大成。簡潔にまとめられた内容は以下の通りです。
(1) Research in Form and Function of the Temporomandibular joint.
(2) Research in Pathologic Joints.
(3) Research in Growth Changes and Effects of Treatment.
(4) Research in Cleft Palate and Breathing.
(5) Research in Prediction.
(6) Research in Cephalometric Analysis.
(7) Further Research in Prediction.
(8) Comparison of Treated to Nontreated Cases.
(9) Research in Function of the Joint, Lips, and Tongue.
矯正歯科臨床では、自然科学の手法の一環として正貌側貌のセファログラムの「計測」を重んじます。むかし講座で彼は話していました‥‥“We have science in order to protect ourselves.”
不可解極まりない言葉ゆえ、深く私の記憶に残りました。いまは、「ほんとうにそうだなァと」と思われる次第(笑)。
と申しますのも、思考が現実認識を逸脱して彷徨う臨床者(歯医者さんだけではありません)に私が多く出会ってきたからでしょう。妄想一歩手前、でも本人は真面目‥‥だから困ったものです。
また、標題が cephalometric とあっても、顎関節(正常像と正常機能&その病理)・呼吸・成長予測(まだ下顎骨の arcial growth 発見前)・歯列や顔の健全な成長の鍵を握る口唇と舌のバランス(今日でも特筆に値する観察と分類)をはじめ、臨床実地を通してしかわかりようのない軟組織と環境因子の影響も幅広く取り扱われています。
そのような意味で、「セファログラム」を軸に、矯正歯科臨床の概要を述べた論説です。
【 Clinical Research 】
〔M.〕 In the continuation of our interview, I know you were requested - I think in 1965(1962) by Bertram Kraus and Richard Reidel - to submit an article to“Vistas in Orthodontics”. Do you want to talk about a little bit about this? Because I think that you said to me before that that sort of gives you a state of the art of orthodontics at that time.
【 臨床研究 】
〔M.〕 インタビューを続けるにあたり、たしか 1965 年(1962 年) のことであったと思われますが、バートラム・クラウス氏、リチャード・リーデル氏から『Vistas in Orthodontics(矯正歯科の展望)』への原稿の依頼をあなたが受けた件について、少しお話なさってはいかがでしょうか。当時の矯正歯科臨床のとりわけバイオプログレッシブについての状況を知る上で、きわめて便宜になる記事であると、以前あなたが話していらっしゃいましたので...。
〔R.〕 Well, I think that I’ve referred to that article because it was a requested article where I had to - well, actually I wrote two articles. First of all was a phone call - or I guess a letter - from Burt, who was a good friend and one that I always admired. And he had asked me to write a paper for a testimony for Alton Moore. And of course, I v’e known Alton for many years and respected him. I said“, Well, I’ll be glad to do. What subject?”“Well, do it on clinical research.”So I said“, Okay.”So for about three or four months, I began to research all of the aspects that entail clinical research of orthodontics.
So I put together an article of about 50 to 60 pages with 88 references. I remember that. And I submitted it and I was pretty proud of it. But they said“, Well this is a good article, but it isn’t what we want. What we would like is specifically the clinical research that you have done, particularly in laminagraphy, cephalometrics, the work you have done to date in orthodontics in diagnosis, and so forth.”So I hitched up my belt and said“, Okay, I’ll do it again.”So I submitted this article, and that was in 1965, maybe late 1964. And it’s rather interesting that that was the same year that I started the advanced courses. So it pretty well represented the status of thinking that prevailed in that year, just when I had started the advanced courses.
In that article, I’d also classified the lips and the three different types of tongue thrusts that we were dealing with in those years. Pretty much the status of the joint and status of growth forecasting in all of that. So if anybody wants to go back and see the status of orthodontics in 1965, get out of that ― 20 years ago now, almost a little bit more ― of what was taking place at that time and the level of our thinking.
〔R.〕 時折セミナーの生徒さんに目を通しておくよう、勧めていたと思います。ことの経緯から説明しましょう。そもそも依頼を受けたのを機に 2 章分の論説としてまとめることになった記事です。依頼が舞い込むに至ったのは、私が親しく尊敬していた友人・バート氏から、電話か手紙か忘れましたが、編集予定の本の中で、"Clinical Research" という章を執筆してもらいたいと頼まれたことに始まります。是非ともアルトン氏(ワシントン大学附属矯正歯科学校の初代校長)の栄誉をたたえてもらいたい、との依頼でした。アルトン氏は私の知己でもありましたから、「喜んで引き受けましょう。でも何について書けば良いのですか?」と私が尋ねたところ、「臨床研究についてです。」と伝えられました。内容をてっきり了解したつもりで、矯正歯科のあらゆる分野の研究を調べ上げ、 3、4 ヶ月かけて、50 ~ 60 頁におよぶ文章を 88 の参考文献を引用する形でまとめました。なかなか上手くまとまったと、我ながら胸をなで下ろしていたのですが、したためた原稿を見せたところ、「困りました。素晴らしい論説なのですが、私たちの望んでいたものではありません。実は他の研究者の業績ではなく、あなたご自身の臨床研究について書いてもらいたかったのです。とくに、顎関節の断層写真やセファロ分析、今まで開発なさってきた矯正歯科の診断などについてです。」と、やんわり戻されてしまいました。そのようなわけで、褌を締め直すことにして初稿から書き改め、1964 年の暮れ、あるいは 1965 年のことでしょうか、提出が終わっていよいよ掲載の運びとなりました。興味あることに、これはちょうど私がセミナー(アドバンスコース)を始めた年に当たります。ですか ら当時の私の思想をよく反映しています。
題材といたしましては、口唇の分類法、3 種類の舌突出癖とその臨床対応、顎関節の研究、長期成長予測法など、当時の全貌を網羅するものです。20 年も前、いや、もう少し昔のことになります。1965 年頃の状況や当時の私の臨床思想を知りたい方は、目を通してご覧になるとよろしいでしょう。
〔M.〕 What were the key issues?
〔M.〕 とくに強調していらした論点は何でしたか?
〔R.〕 Mostly cephalometrics. By now we had begun to feel that there was something about the environment that we could control, rather than treating to it. Open bites were a big problem, always had been. Class III’s with low tongues and cross bites - relapse of open bites and cross bites - were the number one things we had to deal with in orthodontics. So we were addressing those tough situations plus forecasting, and some of the techniques of breaking up the arch and so forth that I had come into at that time. So that pretty much represented what I was talking about at that time.
〔R.〕 多くはセファロメトリックスについてでした。異常なバランス状態に置かれた筋肉や呼吸といった口腔環境に向かって歯を動かすのではなく、口腔環境そのものに対して何らかのコントロールが加えられるのではなかろうか、と感触されてきた頃でしたので、その重要性も強調しました。昔からオープンバイトは臨床の難題でした。低位舌をともなう反対咬合やクロスバイトの治療も厄介であり、開咬、クロスバイトの後戻りも ... これらは、なんとか乗り越えねばならない課題でした。このような臨床上の難局に取り組む重要性について提言したほか、長期成長予測法、あるいはアーチワイヤーを分割して処置する治療手技についても紹介しました。ですから、当時私が話していた内容をよく反映しています。
 |
第8回 An Interview with Dr. Robert M. Ricketts 1987
2016.08.26
第8回:Invisible Progression 克己復禮
Bioprogressive の「Progression」には、いくつかの意味が掛け合わされています。Dr. Ricketts の説明も、質問の趣旨を察しつつ相手に応じて自在なものでした。
丁度、論語三百章のどこにも「仁」の定義づけがないのと同様、「Bioprogressive」もあらゆる定義を一蹴して知らん顔といったところです(笑)。
ところで待機説法に優れていた歴史上の代表人物はやはり釈迦と孔子。その巧みさが災いし、誰かがかってに引き下げた内容ばかりが伝わることになりました。
現在数えればきりのない矯正歯科臨床のなかで(つつまずいえば)最高度の Bioprogressive は同轍を踏むことはない、とは誰にも言い切れません。
ここに、Bioprogressive を創始した Ricketts その人の「克己復禮」の方法論に、我々は直に飛び込んでいかざを得ないわけです。
今回は、専門医の皆様がご自身の臨床の中で「バイオプログレッシブ」なる診療体系を伸びやかに展開する鍵、つまり「思考整序のダイナミクス」について彼自身の言葉からその心裡に迫ってみますが、そのまえに Bioprogressive の「いろは…」を抑えておきましょう。
(1)生物学的原理に基づいて個々の患者さんに最もふさわしい臨床を展開するのが Bioprogressive の特徴なので、ステップ1,2,3…なる治療概念は存在ないこと。
(2)最大非侵襲かつ時間労力といった最大効率を目指すこと。
(3)若年者であれば長期成長予測を行い、Quad helix, Cervical traction, Reverse headgearといったOrthopedicな変化を活用するため 5歳から7歳までの早期から治療を開始するのが望ましいこと。
(4)エッジワイズシステムの活用においては、Light continuos force, cortical bone anchorage, cortical bone avoidance, sectional mechanics, utility arch 等々を活用し、医原性の疾病や医原性の非生理的な適応反応を未然に防ぐこと。
(4)異常な筋バランスに歯を動かすのではなく筋肉の環境そのものへ対応し、ときにはそれを Anchorage へ活用すること。
(5)同様に、歯列と顔の成長には不可欠な呼吸にまつわる生理性の担保につとめること。
(5)標準値からの偏位とその複合原因を把握するための Diagnosis, 自然推移にゆだねたときの Prognosis と治療を行ったときのPrognosis, 個々の患者さんの状況に即した段階的な Treatment planning の立案、治療がはじまってからの Monitoring の5つは、しっかり行うこと。
(6)特定のテクニックに患者さんをはめ込む本末転倒な医療行為は行ってはならないこと。
(6)時々の与件に応じた臨床現場の最適解を判断しする基準として、生物学的原理を援用すること。
(7)自由主義経済のもとで臨床活動を継続させるために、実経験にもとづく知性と幅広い人間性をやしない、行動社会学や心理学といった対人関係の構築に有益な学問も活用すること。
(8)患者さんのモチベーションを高める努力を怠らないこと。
・・・あげればきりがありません(笑)。ですから、現行の他の治療システムと同次元で論じるのは無理があります。
ところで、1991年のAdvanced course のなかで、彼は
「Bioprogressive is a wedding of progression with biology. So, it’s actually biologic progression. The application of bio-mechanical principles in a sequence with a pre-determined hierarchy in order produce the maximum benefit with minimum of effort, of course, with the least amount of tissue damage.」と説明していました。一見整っているものの歯切れ悪さが残りました。でも一般説明としては申し分ない。
しかし再応、我々が知りたいのは、それを日々創造するための「奥底」なのです。
Copyright © 2015 University of Michigan School of Dentistry
Some rights reserved. Except where otherwise noted, this work is licensed under the following:
Attribution: Please attribute the work to the University of Michigan School of Dentistry and any individual author(s) cited. Not-for-profit: Use, display, and redistribute all or part of this work for non-profit and educational purposes only.
Share alike: Redistribute derivative works with the license listed here.
Visit the University of Michigan School of Dentistry’s website at http://www.dent.umich.edu/.
View the original interview at https://www.youtube.com/watch?v=lcBLmVOn3m0.
Interview conducted by James McNamara, DDS, MS, PhD. Interview transcribed by Yuri Shindo, MD.
Interview translated by Katsuyuki Shindo, DDS, PhD.
【 Invisible Progression 】
〔M.〕 Ok, we’re just about running out of time on this segment. Do you have any other comments that you want to make along the line of the things that we’ve talked about?
【 克己復禮 】
〔M.〕 今の話題に関してはあまり時間がないのですが、付け加えておきたいコメントはありますか?
〔R.〕 About these developments? Well, I think that about two years ago my family and I went to Sun Valley, Idaho for Christmas vacation. Everybody else was out on the slopes, but I was sitting there babysitting. It had to be more than two years ago, rather a few years back. I started to put together all of the changes that I had made since the start of my experiences in orthodontics. A change in philosophy, or a change in technique. I started to list them, and it grew to a list of 278. So I have shifted somehow in technique or philosophy 278 times in these 40 years.
〔R.〕 これらの進歩についてでしょうか? 2 年ほど前、いや、もう少し前になりましょうか... クリスマス休暇で家族とアイダホ州のサンバレーに出かけたときの出来事です。家族の者がスキーを楽しんでいる間、 私は子どもをあやしながら自分が矯正歯科の世界に入って以来、考えや技術に関していったいいくつの改革を重ねてきたか、一つ一つ数え上げていきました。すると 278 項目にも及んだのです。技術と臨床体系の考えを、ここ 40 年間にわたって 278 回も刷新していった事になります。
〔M.〕 So the Ricketts of 1966 is not the Ricketts of 1987?
〔M.〕 ということは、1987 年の今日のあなたは、1966 年の R. M. Ricketts と別の人物ということですね。
〔R.〕 Not at all. Things have changed since people took my course fifteen years ago, ten years ago, or even two years ago. It’s been a progressive change all the way through as new ideas come along. A lot of times I’ve made an investment in an old idea, but I have to give it up. You can’t stand where you are if you’re going to proceed. You can’t stand still.
〔R.〕 その通り、全く違う人間だということです。2 年前のコースの内容は今とは違うし、況んや 15、10 年前とははるかに違います。新しい概念が生まれればそれを検討し、それに呼応して我々はプログレッシブに変化を続けていくだけです。幾度も新たな考案を検討し、それが無効と判断されれば棄て去る... それを繰り返していきました。現状に満足したらもはや進歩は望めません。立ち止まっている暇など、医療者には本来はないのです。
〔M.〕 Ok, thank you.
〔M.〕 ずばり、ご尤もですね。
 |
第7回 An Interview with Dr. Robert M. Ricketts 1987
2016.08.24
第7回:The Birth of Bioprogressive バイオプログレッシブの産声
Copyright © 2015 University of Michigan School of Dentistry
Some rights reserved. Except where otherwise noted, this work is licensed under the following:
Attribution: Please attribute the work to the University of Michigan School of Dentistry and any individual author(s) cited. Not-for-profit: Use, display, and redistribute all or part of this work for non-profit and educational purposes only.
Share alike: Redistribute derivative works with the license listed here.
Visit the University of Michigan School of Dentistry’s website at http://www.dent.umich.edu/.
View the original interview at https://www.youtube.com/watch?v=lcBLmVOn3m0.
Interview conducted by James McNamara, DDS, MS, PhD. Interview transcribed by Yuri Shindo, MD.
Interview translated by Katsuyuki Shindo, DDS, PhD.
【 The Birth of Bioprogressive 】
〔M.〕 Now when did the term “bioprogressive” come into existence?
【バイオプログレッシブの産声 】
〔M.〕バイオプログレッシブという呼称はいつ生まれたのですか?
〔R.〕 By 1958, we started treating Class II’s with second order bends. By the time that I started my practice in 1952, and with the studies that I had done, I found that that was nonsense. In theory it would work, but in practicality it didn’t. It just couldn’t be controlled the way that we had anticipated, and we ended up with this displacement. It was locking the upper arch more than anything else. It was locking it so that it couldn’t respond.
I have to give Chad Rye up in Indiana a great deal of credit for my whole career. When people ask me who I think are the greatest orthodontists that I’ve seen, I say“, Well, there are two men that I always felt were the tops.”If it were an extraction case, it would be Hayes Nance. He paid more attention to detail in extraction than anybody I ever saw, even among orthodontists today. The guy who was the best technician for non-extraction cases was Chad Rye in South Bend. In fact, he went to Michigan. Did you know that? He took the Dewey course too. But the first time I saw him work was when he was using sliding hooks on steel wires. He later started to use .021 × .021 inch steel wires so he could slide the teeth down.
Well, my studies indicated that even this was going to tip the whole occlusal plane because there’s a force as long as you had that with the incisors banded and engaged. The force is going to do this to the upper arch, and it’s going to extrude the upper incisors. So one day I had these arches in. I just went in and cut the wire in here. I said, “Let’s see what happens if I leave these up here and bow this side and put intermaxillary elastics just off and above these segments.”So one day, clip clip. Next patient, clip clip. Next one, clip clip. So I had a whole series of patients in which I was taking buccal segments back independently. That gave rise to the understanding of the forces that were operating through this part of the arch. The next thing that I ran into was this business of separation, which always bothered me.
〔R.〕 1958 年まで、セカンドオーダーベンドを加えてからII級関係の修正をはかる治療を我々は行っていました。しかし私は開業する 1952 年以前に、独自の研究を踏まえて、これは無意味であるとの結論に達していました。理論上は有効に見えますが臨床ではそうはならない... 期待通りコントロールすることは無理であり、どうしても位置がずれ起こってしまいました。(海面骨の豊富な)上顎に一番の固定源を求めるものですから、思い通りにことが運ばないのは当然だったと思われます。
ところで、私の生涯で高い信頼をおいている臨床家にインディアナ州のチャッド・レイ氏がいます。今まで出会った中で偉大な臨床家は誰かと問われれば、「二人の人間がトップでしょう」と私は答えています。抜歯治療ならヘイズ・ナンス氏。細部にわたり細心の注意を払う彼の右に出る人は、今なおいません。非抜歯治療ならサウスベンドで開業しているチャッド・レイ氏を挙げます。ドゥーウィ氏の講座を受けに彼がミシガン大学に来訪していたことをご存じでしたか? 初めて(チャッド・レイのオフィスを) 見学した折、スチールワイヤーにスライディングフックをつけて治療しているのを見かけましたが、後に彼は .021 × .021 inch のスチールワイヤー上で歯を滑らすテクニックを採用していました。
ところで、私がセファログラムで治療変化を調べていた時のことですが、上顎前歯にバンドを装着してフルアーチで顎間ゴムをかけると、咬合平面が傾斜してしまう反応が起きているのに気づきました。そこである日、アーチワイヤーの途中を切って側方歯群をセグメントに分割し、そこへ顎間ゴムをかけてみることにしました。装着中のフルアーチワイヤーを「パチン」と切っては、次の患者も、またその次も同じようにワイヤーを分割しました。こうして頬側セグメントを単独に遠心移動させたのです。お陰でこの領域のコントロールにまつわる力の加減がだいぶ把握できました。次に取り組んだのは、面倒なセパレーションの簡略化です。
〔M.〕 What do you mean by“separation”?
〔M.〕 なにをセパレーションするのでしょう?
〔R.〕 Separation of all of the teeth, and placing them in an appliance. I started putting molar bands on and only canines here. Molars here and canines here. I started moving teeth by intruding canines with this and I saw the molar back up. So I started banding teeth in a progressive way. That’s where the word“progressive”came from.
I started doing this in 1952. By 1955 I had started using preformed bands, and by 1958 I had worked out all of the preformed bands. My typodont for the American Board in 1958 was the first one that was all done with preformed steel bands. I had premounted the tubes rather than just the brackets, and worked it out to the level of the margin of the band rather than the height of the bracket [the cusp height to the slot of the tube] This technique was highly efficient. I could band up a case - I’ve proven it with a stopwatch - in fifteen minutes for a full mouth. I mean, that’s incredible!
〔R.〕 すべての歯牙の隣接面を離開させて装置を入れるセパレーション作業のことです。大臼歯と犬歯だけにバンドを装着しました... こんなふうに。次に犬歯を圧下移動させ、大臼歯をティップバックさせます。すると隙間が歯と歯の間に広がっていくので、徐々にバンドを装着できるわけです。これがそもそもの「プログレッシブ」なる言葉の由来です。
1952 年からこの方法を採用し、1955 年までには既製バンドを使いはじめ、全ての歯(上下第二大臼歯は除く)にわたる既製バンドを 1958 年までに完成させました。同年開催された全米歯科学会では、このスチール製のバンドをタイポドンントにまとめて装着する作業を実演してみせました。バンドにはあらかじめブラケットが電気溶接されており、スロットまでの高さは従来のように咬頭頂を基準に決めるのではく、辺縁隆線の高さを基準にしました。効率の観点から素晴らしい成果を収め、ストップウォッチで作業時間を測ると(上下第一大臼歯間の全てのバンド合着が)僅か 15 分... 驚異的な速さでした。
〔M.〕 How long would it have taken you before?
〔M.〕 それ以前はどのくらいの時間がかかっていましたか?
〔R.〕 Two hours. So that’s one-eighth of the time that it would have taken before.
〔R.〕 2 時間です。効率からみて 1/8 に時間を短縮したのです。
〔M.〕 Do you think that if bonding had been available when you started, then a lot of -
〔M.〕ボンディング技術が使える時代ですから、そちらを使ったらもっと...。
〔R.〕 I’d have still been progressive because if I hadn’t gone through this technique, I wouldn’t have understood what you could do with a molar from four lower incisors. That happened in 1963. The utility arch was born as a result of experimental orthodontics, followed by cephalometrics. Of course, in those days I did my own head films and I was racing. I was taking them all the time.
In 1958, I was the guest speaker for the European Orthodontic Society, and a guest of Arne Björk. A lot of people asked me what technique I was using, and I said“edgewise.”Well, I realized that the image that they had of edgewise was Tweed edgewise, and that was all. They didn’t understand the versatility of multiple brackets on teeth, and the versatility that you had with lighter forces. I realized at that time that I had to have a new label.
In the beginning, I called it the“light square technique”. But it wasn’t always light, and it wasn’t always square. I was using a progressive technique. In 1966, I had one of my early classes and I said, “Well, you’ve all seen what I’m doing here and you know that it’s different. It’s not what we have seen as traditional edgewise, which was the primary, secondary, or tertiary edgewise, which was Tweed edgewise.”I said“, What are we going to call this?”I called it a progressive technique. That was the class that Tom Christie was in, and that was a very alert class. That group was one of the most outstanding that I had in 1966. We were meeting in my home, sitting around on the floor after dinner, and discussing the course - we used to call it The Last Supper. They said“, Well, we’ve been thinking about this and we think that the word‘biology’should be represented.” So right on the spot, we said “bioprogressive”, and looked around the room. Everybody agreed. So that’s when the word, “bioprogressive” was born.
〔R.〕 私はバンドを用いたバイオプログレッシブ法(※ 徐々に歯間 部を開けてバンドを合着してゆく手法)をやはり選択します。というのも治療技術が発展してくる過程を顧みれば、この筋道を通らない限り、大臼歯を用いて下顎前歯を三次元にコントロールする技術(= U/A の考案)は確立し得なかったからです。1963 年の発見でした。セファロを検討しながら試行錯誤を重ねた結果、ユーティリティアーチが誕生しました。その頃はセファログラムを一枚一枚手でトレースしていたので時間に追われていました。しかし、これが幸いして歯列の変化が把握できたのでしょう。
ところで、アーン・ビョルク氏の招きでヨーロッパ矯正歯科学会の特別演者として出かけたのが1958 年です。多くの人々からどんなテクニックを使っているか尋ねられたので「エッジワイズ法です」と一応は答えたものの、彼らが思い描くのはツイード法によるエッジワイズシステムばかり...。それ以外の発想はなかった様子です。今から思えば説明に苦慮して当然でした。同じマルチブラケットでも、用法や使い方次第では穏やかな力を発揮させたり、為害性の少ない処置が行い得る融通性について、彼らが理解しているようにはとても見えませんでした。そこで、新たに名前をつけようと思い立ったわけです。
はじめ、「弱い力の角線システム」と呼んでいましたが、常に弱い力を作動させるわけではありませんし、また角線のほかに丸線も併用します。しかし、「治療上の必要な順位を探し、段階的に治療を開始し、徐々に装置を外していく」、といった個体差に応じた段階的なアプローチの概念はあらゆる患者に共通していました。そこで1966年のコースで生徒にこう尋ねてみたのです... 「ここで私がやっていることが伝統的なエッジワイズシステムと違うものであることを皆さんはご覧なりました。「第一世代」や「第二世代」とも、そして「第三世代のツイード法」とも異なります。どんな名称がふさわしいか、ご意見を下さい。」当時は「プログレッシブテクニック」と私なりに呼んでいました。際だって聡明なそのクラスの中にトム・クリスティー氏がいました。コースを終えて自宅に生徒を招き、夕食後、床に座り込んでコースのことをいろいろと振り返る機会を設けていました。戯れにこれを「最後の晩餐」と呼んでいたのですが...(笑)。「ちょうどそのことを相談していたところです。『生物学』という言葉がそこに反映されていることが大事だと思います。」即座に『バイオプログレッシブ』がぴったりだと閃いたので、生徒たちに意見を聞いて見渡してみたところ、皆納得した様子でした。「バイオプログレッシブ」の誕生です。
 |
第6回 An Interview with Dr. Robert M. Ricketts 1987
2016.08.19
第6回:A New Art 歴史をふまえて
Copyright © 2015 University of Michigan School of Dentis-try
Some rights reserved. Except where otherwise noted, this work is licensed under the following:
Attribution: Please attribute the work to the University of Michigan School of Dentistry and any individual au-thor(s) cited. Not-for-profit: Use, display, and redis-tribute all or part of this work for non-profit and educa-tional purposes only.
Share alike: Redistribute derivative works with the li-cense listed here.
Visit the University of Michigan School of Dentistry’s website at http://www.dent.umich.edu/.
View the original interview at https://www.youtube.com/watch?v=lcBLmVOn3m0.
Interview conducted by James McNamara, DDS, MS, PhD. In-terview transcribed by Yuri Shindo, MD.
Interview translated by Katsuyuki Shindo, DDS, PhD.
【 A New Art 】
〔M.〕 Well, you know Bob Aldrich still practices in Ann Arbor and he’s told me many times about being in your first course. Now, you mentioned that you were a source of controversy. Having personally also been in that spot oc-casionally, I can relate to that. When you came out of Il-linois in 1952, what were the existing or pervasive para-digms in orthodontics? Where did you deviate?
【 歴史をふまえて 】
〔M.〕 ご存じの通り、ボブ・オードリッヒ氏はアンアーバーで診療をしていますが、第一回目のリケッツコースを受けたことをよく話してくれたものです。先述の話では、あなたは論争の嵐の目になっていたとのことですが、そのような場にたまたま居合わせる機会が私にもありましたので、その様子が思い浮かびます。イリノイ大学を 1952 年に離れたとき、 矯正歯科界に充満していた理論は、どのようなものだったのでしょうか。また、あなたがそれらの潮流の、どの辺りから離れていったかもお聞かせ下さい。
〔R.〕 As you know, the edgewise system was born in the 1920’s. It precipitated in 1928 and 1929, and Angle died in 1930. His students took over, and they had this marvel-ous mechanism which allowed them to control and band all the teeth. So the initial theory was that you should be able to treat the entire malocclusion in the time that it took to treat the slowest responding tooth, which was the molar. If you could correct the molar relationship with intermaxillary traction in three months, then you should be able to do the whole thing in three months. Now that sounds incredible, but in 1928 Brodie published an article on the rapid treatment of Class II Division 1. Can you be-lieve that he was advocating treatment in three months or even less? He said, “We shouldn’t say that we can get all cases treated in that time any more than we can treat all cases in ten months with the ribbon appliance.” So they were treating cases in ten months with the ribbon ap-pliance. Now that’s incredible in terms of what we do to-day. I mean, I would no longer think of trying to achieve that because that’s as unbiologic as can be. Don’t for-get that Ray Begg was also trained in this primary edge-wise philosophy.
Even when I was a student, we took six months to set up the anchorage, so to speak, to get each arch individual-ized. We took three months with intermaxillary elastics. We were finished in nine months. Even when I was in school in 1947, our goal was to get our cases treated. Ours was the first class that invested over one year in orthodontic graduate work. We went eighteen months.
〔R.〕 エッジワイズシステムは 1920 年代に生まれ、1928 年から翌年にかけてにわかに普及、1930 年にアングルは他界しました。弟子は彼の遺志を継いで、すべての歯牙にバンドをとりつけてコントロールするこの驚異的なメカニクスを治療に導入しました。不正咬合の種類を問わず、全治療期間は一番反応の遅い大臼歯の修正が完了するまでの期間であるべきであると当初は考えられていました。そして 3 ヶ月間以内に顎間ゴムで臼歯関係を是正できるなら、すべての治療は 3 ヶ月で終わるだろう... そう単純に思い込んだのです。じつに飛躍した発想なのですが、1928 年にブローディ教授はII級 1 類の迅速な治療について論文を刊行しています。その中で彼は僅か 3 ヶ月、症例によってはそれよりも短い期間で動的処置が完了すると述べています。しかしさすがに一方で、こうも付け加えていました ... 「すべての症例が、リボン型装置を使った場合の 10 ヶ月よりは短くて済むなどと、口が滑っても言ってはならない。」つまり、リボン型装置では 10 ヶ月で治療を完了していたことになります。今日の我々の知見に照らすと馬鹿げています。生物学的には全く受け入れられないので、安易な期間の短縮に挑んでみようなどという気は、私には毛頭ありません。レイ・ベッグ氏も、この初期のエッジワイズ学で訓練を受けた弟子のひとりであったことを皆さんは覚えておかれると宜しいでしょう。
私が入局していた頃ですら、上下の歯列を各々の理想形状へ近づけるアンカレッジの準備に 6 ヶ月を費やしていたのです。そのあと 3 ヶ月をかけ、顎間ゴムを使いながら前後の関係を整えようとしていました。ですから治療期間は合わせて 9 ヶ月でした。1947 年当時はこれを治療期間の目標に掲げていました。ちなみに初の試みとして、卒後臨床教育期間を 1 年 以上に延長して、18 ヶ月にしたのが私たちのクラスです。
〔M.〕 Alright, you’re telling me some stuff that, I guess with me
maybe being slightly younger than you, I haven’t really heard that much. Let’s go back to that again. You’re telling me that you’d set up a case for six months. This would presumably be a non-extraction case, right?
〔M.〕 先に何名か、あなたより少し若い医局員らのことをお話しなさいましたが、私にはほとんど初耳でした。ともあれ、6 ヶ月で (アンカレッジの)準備を完了することに触れていらっしゃいましたが、非抜歯治療でしょうか?
〔R.〕 Yes, and under Brodie we learned non-extraction. I call that the“primary edgewise”. Then I had secondary edgewise, then tertiary edgewise, and then bioprogressive. So I went along that chain in the development of what we’re doing today.
〔R.〕ブローディ教授の許では非抜歯治療を学んでいました。これを「第一世代エッジワイズ法」と私は呼んでいます。やがてエッジワイズ法は「第二世代」、「第三世代」、そして「バイオプログレッシブ」へ発展していきます。私自身このような変遷過程を経験しましたが、今の我々の臨床もその一連の上に存在しています。
〔M.〕 Now how did a change in molar relationship occur in three months?
〔M.〕どうやったら、たった 3 ヶ月で臼歯関係を変えられるのでしょう?
〔R.〕 With intermaxillary traction.
〔R.〕 顎間ゴムを用いて変えます。
〔M.〕 But it was strictly tooth movement?
〔M.〕 ということは、歯牙だけの移動ですか?
〔R.〕 Strictly tooth movement.
〔R.〕 まさにその通りです。
〔M.〕 How many ounces or pounds of force?
〔M.〕 そのときの力は?
〔R.〕 When I went to school, we had the old rubber elas-tics - the gum rubber - and the patient changed them every day because they got soggy. We applied second order bends to progressively tip back the upper molar, even to the ca-nine, and this was supposed to be activated by an intrud-ing force against the upper incisor. Don’t forget, it was only in 1938 that they did the first analysis of cases treated with that appliance.
The edgewise appliance is what entered all of these limi-tations into orthodontics in my opinion. Well, it’s not just my opinion, but rather a fact that this is the way things are going. How much could you intrude teeth in three months with a continuous arch? How much could you enjoy growth? How could you do anything other than move teeth in three months? Now, if you’re going to open a bite by mandibular rotation and you’re going to treat a case by displacing the lower arch forward, you’re going to end up with a double protrusion. It’s not going to look good, it’s not going to retain well, and it’s going to end up with a face full of teeth. Well, that’s what Tweed was trained in. It wasn’t three months, even in the secondary edgewise that I got.
〔R.〕ガムラバーという旧式のゴムバンドを使っていましたが、すぐふやけてしまうため毎日交換しなくてはなりませんでした。セカンドオーダーベンドを入れて上顎大臼歯を徐々に遠心に傾斜させ、実際には犬歯までも遠心へ倒しました。セカンドオーダーベンドの反作用で上顎前歯には圧下力が働くことになっていたでしょうが...。この方法による治験症例の解析が (セファログラムを用いて)なされたのは、1938 年であったことを念頭におかねばなりません。
当時のエッジワイズ装置は、私の謂う「教条的制約(思い込みによる治療限界)の時代」へちょうど突入したところでした。私見というより、 事実とみなしてよろしいでしょう。連続アーチをつかって、僅か 3 ヶ月の期間にいったいどれ程の歯の圧下移動が期待できるのでしょうか? いかほどの成長が見込めるというのでしょうか? 慌ただしく 3 ヶ月で歯を動かすほかに、なにか出来ることがあるのでしょうか? 咬合挙上のため、下顎を後方へ回転させ、下顎歯列全体を前に滑り出させるわけですから、上下歯列前突(長顔下顎後退型の上下歯列前突)を招くだけです。見た目は悪いし(顔の垂直高径は人為的に不調和を来たし)、保定中の安定も優れない、おまけに顔の中で歯がやたらと目立つことになります。ツイード氏はエッジワイズ法で訓練を受けた臨床家、つまりこの不都合に直面したわけです。なお、期間について付言するなら、私が経験した「第二世代エッジワイズ法」では、もう 3 ヶ月で動的処置を済まそうなどという発想は消えていました。
〔M.〕 Now what was the difference between the primary edgewise -
〔M.〕 初期型、すなわち「第一世代エッジワイズ法」とそれ(「第 二世代」)とは、どう違っていたのですか?
〔R.〕 With the primary edgewise technique, you put the in-termaxillary elastics on the day you start the case. So you separate, separate, separate, put the whole appliance in, adapt an 0.022 × 0.028 in an 0.028 bracket ‒
〔R.〕 「第一世代エッジワイズ法」では治療開始直後から顎間ゴムを使い始めました。歯間部を次々とセパレーション (真鍮線を歯間部に入 れて歯間分離)して、全部の歯にバンドをとりつけ(スロットの幅は 0.028 in.)、そこに合うように曲げた 0.022 × 0.028 in. のワイヤーを挿入し...
〔M.〕 Made of gold wire?
〔M.〕 金合金ワイヤーでしたか?
〔R.〕 Yes, gold wire. And take out the appliance for every adjustment. You saw the patient every week to every two weeks. Back then, there weren’t any monthly visits. We saw the patient at least every two weeks. So you were mov-ing teeth as rapidly as the patient could tolerate.
You put stops on the molar tubes on the wires, then put a washer in, to advance the wires to make more space. If the teeth were crowded, you’d continue to tie them in. Any time you have a complete unit, the one that’s going to move is the one that’s the weakest. It’s like a stave around a barrel; the pressure will be the same everywhere on that stave. Well, arch wires are the same. So expansion became synonymous with forward movement of the lower inci-sor because that was the weakest tooth and it would be the one that would get displaced. Any time that an edgewise orthodontist thought of expansion, he immediately thought of forward movement of the lower incisor. So that would stress it once.
Then while you were expanding the arch, you would also put intermaxillary elastics on which would push the molars out of root position. There was nothing to hold them so the lower arch“blew”and you duct it on the occlusal plane.
Tweed started showing that he could treat patients with extractions. He would go in, take four teeth out, and bring the teeth back. He treated all of these patients at his own expense, and had become a hero. He became a hero because a lot of people had seen the same thing. People saw this as a vehicle to achieve their treatment goals. In my opinion, this was the evolution of the whole era which we call the“Doctrine of Limitations”. That’s what I saw, that’s what I experienced. Don’t forget that I came into orthodontics in 1947. That was the year that Hays Nance [1893-1964] wrote his article, “The Limitations of Orthodontic Treatment”, which incidentally was written by Wendell Wylie. Did you know that? It was Nance’s materi-al, but it was written by Wylie. I don’t know why his name wasn’t on it. The following year, Strang [1881-1982] wrote the article“, The Fallacy of Denture Expansion as a Treatment Procedure”. Here’s the guy who wrote the orig-inal work on expansion - who wrote the book in 1935 on edgewise technique - and suddenly after twelve years, he completely goes to the other side. He was praising Tweed, and agreeing that you could not really expand cases. So this was the era that I came into.
I came along with my own technique using laminography and growth forecasting, and I had to cross the Tweed group in Southern California which was probably the strongest group any place. At that time the society included Charles Tweed, Hayes Nance, Roscoe Keedy, Cecil Steiner. When I started opposing extraction, and started putting in canine rises - because at that time you were supposed to take out cuspids and put them all in group function - I got into problems in occlusion.
Everybody was in this tie back, tie back, tie back busi-ness of very vigorous forces. When I started talking about lighter forces and then later went into progressive band-ing of cases rather than getting all of the bands on at once - moving teeth out of the way by moving teeth, in-truding teeth, and so forth rather than by separators - that was strange to them. So I had that problem. Nobody believed that you could get a condyle back too far in those years. Nobody. One of the best known clinicians called me one time and said“, Rick, I think you’re all wrong in this.”I said,“Wrong in what?”He said“, I’ve never seen a condyle back too far.”What was I going to say?
Don’t forget, when I went to California there were only five cephalometers in the state, and two of those were in institutions. Nobody was using cephalometrics at that time. I remember one of my colleagues said to me once over a beer“, Tell me what you can really see with cephalomet-rics that we can’t get with our models and our photo-graphs.”So that was the prevailing climate in 1952 when I went to California.
〔R.〕 そうです。金合金ワイヤーです。毎回の来院時に調整を加えていきました。来院間隔は毎週もしくは隔週でした。ひと月に 1 回の来院ではなく、最低でも 2 週間に 1 回はワイヤーを口腔外で調整してはまた戻しました。患者が痛みに耐えられる限界まで大きな力をかけ、とにかく迅速に歯を動かそうとしました。
大臼歯のバンドにとりつけたチューブの近心にストップベンドを入れ、ワッシャーを徐々にワイヤーにかませていき、前歯をアドバンスさせていきます。これで歯列弓の長さは増し、歯と歯の間に隙間もできてくるので、叢生が残っている歯を外側に引っ張り出すように結紮を強化し、歯列を整えるわけです。ところが歯列全部をまとめて整えようとするこの術式には、とんでもない落とし穴が潜んでいました。支持の弱いところばかりが先行して動いてしまう問題です。ちょうど、樽(歯列)の横板(歯) を外側に回した針金で隙間をつくりながら並べようとするようなものです。分散された力は、横板へ均等に働くとはいえ、脆弱な部分に力は集中します。唇側の皮質骨が皮薄で歯根の細い下顎前歯が、この脆弱な横板に相当します。したがいまして、エッジワイズシステムを扱っていた矯正歯科医にとって「拡大」という言葉は、「下顎前歯の前方傾斜」と同義に錯覚されたほどでした。それが一点です。
さらにこの操作中に顎間ゴムをかけるのです。下顎大臼歯は拡大のメカニクスによって頬側へ傾斜しますが、これは歯根が皮質骨を外れて海面骨の中へ入ってしまうことを意味します。つまり大臼歯(アンカレッジとして)の安定性がすっかり失われた状況を招くのです。そこへ顎間ゴムをかけると、不安定極まりない下顎歯列はいともたやすく咬合平面に沿って急激に飛び出てしまったわけです。
そこでツイード氏は 4 本の小臼歯を抜去して前歯を後ろへ牽引する治療を公開しました。再治療の費用は彼がすべて負担したので、時代の英雄に一躍躍り出ました。同様の帰結に悩んでいた多くの人々は、ツイードの術式を目にして、「これなら目標に到達できる」と歓喜しました。矯正歯科における最大の「教条的制約」はこうして生まれたと私は睨んでいます。しかも、矯正歯科史を通してもっとも強いインパクトを人々に与えたと思います。1947 年にこの分野に飛び込んだ私が、実際この目で見て、そして経験してきたことなのです。ヘイズ・ナンス氏は同年、「矯正歯科治療の限界」なる記事を書いているのですが... もとは彼の論著なのに、ナンスの 名が併記されずにウェンデル・ワイリー氏の研究として刊行されたのは訝しく思われます。それはそれとして、翌年ストラング氏が『治療段階としての歯列拡大の誤謬』なる記事を執筆しました。もとは 1935 年にエッジワイズ法に関する著作で歯列拡大を述べていた彼が、こともあろうに 12 年後、正反対の立場に転向してしまったとは驚きです。ツイード氏を賞賛し、歯列の側方拡大処置は放棄してしまいました。私が矯正歯科臨床に携わるようになった時代の風潮は以上の通りです。
そのような中、全米で最大の勢力を誇るツイードグループの本拠地南カリフォルニアに、彼らの治療に異を唱えるべく、顎関節の断層撮影と長期成長予測法を駆使した独自の技術を携え私は乗り込んでいったのです。当時のツイード学会はチャールズ・ツイード氏、 ヘイズ・ナンス氏、 ラスコ・キディー氏、セシル・シュタイナー氏らそうそうたるメンバーを擁していました。(ツイード法で提唱されるような)抜歯治療に異議を唱え、犬歯を直立化させる処置を私は開始しました。というのも犬歯の重要性を考えずに犬歯を抜去してグループファンクションに仕上げる治療法すら散見され、私にとっては咬合の考え方そのものにも疑問が抱かれたからです。
すべての人がタイバックを繰り返し、きつく歯列を締め上げる処置をしていたさなか、弱くて持続的な力を私は提唱し、また一度にすべての歯にバンドを装着する方策を改め、歯と歯の間におのずとスペースが生まれる状態に整えてから(下顎の犬歯と大臼歯のみにバンドを装着し、犬歯を圧下移動しつつ大臼歯を遠心へ動かして小臼歯間スペースをつくり出す方法など)無理なく徐々にバンドを装着しました。彼らから見れば、さぞかし奇妙な術式に映った様子で、説明に窮しました。当時は顎関節内で下顎頭が後ろの位置に収まっている治療結果など、到底信じられなかったわけです。著名な臨床家がクリニックを訪ねて来た折の会話を思い出します ... 「リック、あなたがやっていることは全部誤っているのでは?」、「どうしてですか?」、「だって治療後に下顎頭が関節窩の後ろに収まったままの症例にお目にかかった事など、かつてなかったものですから。」... これには返す言葉が見つかりませんでした。カリフォルニアに私が行ったとき、州全体でセファロの撮影装置は 5 台、うち 2 台は研究機関にあったような状況で、誰も臨床に活用してい ないのも同然でした。矯正歯科仲間のひとりが、ビールの酔いに任せ、「写 真とか歯列模型以外で、セファログラムじゃないと分からないものがある というなら、貴様しゃべってみろ!」とからまれたことを思い出します。これが1952 年、私がカリフォルニアに渡った頃に蔓延していた矯正歯科の潮流です。
〔M.〕 Tell me about the interaction between Brodie and Tweed.
〔M.〕ブローディ教授とツイード氏はどんな反応を示しましたか?
〔R.〕 ...he was no longer putting on intermaxillary elas-tics at the start. He was beginning to take longer to treat patients. Having taken his practice for two summers when he was gone on vacation, I knew what he was doing. He didn’t even treat his cases as fast in his practice as we did in school. So he had to treat cases faster at school in order to give students enough exposure. Based on what I saw in his practice, he extracted teeth in about 15% of cases. The technique that he used for extraction, when he did so, was to go in and level the arches as we had typi-cally done. He would take out the bicuspids, and use noth-ing but tiebacks.
As you and I both know, that’s going to displace the low-er molars forward rather rapidly, but that’s the way a lot of extractions were done, even with Tweed who used vigorous forces before he went to Class III elastics. So that was what was happening in the 1930’s.
When Angle entered the field of orthodontics, the pendulum was all the way on the other side toward extraction. All Class II’s were treated by extraction of the upper bicus-pids and movement of the upper incisors back over the low-ers. All Class III’s were treated by extraction of the lower bicuspids and bringing them in under the uppers. That was the status of orthodontics when Angle came into the field. In about 1895 or 1898 - sometime just before the turn of the century - he found the Baker anchorage. He also found that intermaxillary elastics could correct a whole arch. Nobody thought that just a light little thin intermaxillary elastic would be strong enough to move a whole arch of teeth. But when that was discovered, they began to employ it. Angle saw that as a vehicle to treat patients without having to extract teeth.
He also advocated starting treatment at a young age, which is something that a lot of people don’t know. Even in 1926, he used the baby ribbon appliance which was designed for deciduous teeth. Did you know that? 1924. That was ac-tually the interim between the ribbon and edgewise appli-ances. He didn’t go from ribbon to edgewise in one jump. There was an interim appliance called the baby ribbon. Most people don’t know about it. Spencer Atkinson helped him work it out. That’s where they had their clash. Then Atkinson went on to design the universal appliance, and Angle the edgewise appliance. That’s how the clash oc-curred. Both of them got patents during the same year, 1928. Did you know that? That’s what happened.
So this was the status of orthodontics when I went to Cal-ifornia in 1952. So at that time, they had not yet started using extra-oral traction as a rule. They were following Tweed and there were just the beginnings of extra-oral traction when I first went there.
〔R.〕 治療開始直後から顎間ゴムを使うことはなくなりました。彼はもっとゆっくり処置をすることを心がけるようになりました。ブローディ教授が二度の夏期休暇で外出しているとき、彼の診療所に代診に出かけ、そこにおける治療が医局のといささか違うことに気がつきました。ひとつは先述の通り、急がない治療です。技術面で生徒の指導をしなければならない都合上、大学では急速に歯を動かしていたわけとなりましょう。個人診療所におけるブローディ教授の抜歯症例は、私のみた限りでは全体の 15%。その術式は典型例と同じく、まずは歯列をレベリングし、小臼歯を抜去、あとはタイバックだけでスペースを閉じるやり方でした。
ご存じの通り、従来型の術式では下顎大臼歯が容易に前へ滑ってしまいますので、当然ながら小臼歯抜去が頻繁に行われるようになったのです。強力な力を用いていたツイード氏も然りです。彼の場合はIII級ゴムをかける術式に変更する以前には、大臼歯の皮質骨固定を崩すほどの強大な力を付与してしまっていたのです。1930 年代はこのような時代でした。
アングルが矯正歯科界に登場したときの状況は 1930 年代と似たり寄ったりで、抜歯非抜歯の思潮的なうねりを振り子に喩えるなら、抜歯治療に大きく振れ切ってしまった時代でした。すべてのII級症例は上顎小臼歯を抜いて上の前歯を後退させ、III級なら下顎小臼歯を抜いて下の前歯を後ろへ... そんな単純な治療法がまかり通っていました。1895、8 年頃だと思いますが、とにかく 19 世紀の終わりにアングルはベイカーのアンカレッジに着目し、顎間ゴムの作用で上下歯列全体が動くことを発見しました。微弱な力の小さな顎間ゴム... それがこれほどの変化をもたらすなどとは誰にも思い寄らなかったのです。アングルはこの着想に力を得て、非抜歯治療が可能になる例を経験し、このことが明らかになると普及に努めました。
また、彼は若年期に治療をはじめることの有用性を説いた人でもあります。広くは知られていませんが、乳歯列用に開発されたベイビーリボンというシステムを考案、1924 年に報告しています(※“Special Mechanism for the Treatment of Deciduous and Mixed Dentition.”Angle EH. 1924)。リボンアーチとエッジワイズ法の移行期に使われていました。リボンアーチシステムからエッジワイズ法へ跳躍したのではなく、移行段階があったのです。そがベイビーリボンですが、そのいきさつを知る人はもう稀です。ところで、アングル校において講師として彼を補佐していた人にスペンサー・アトキンズ氏がいます。アトキンズ氏はユニバーサル装置の開発に向かい、アングル氏はエッジワイズ装置へと向かったのを機に、両者はついに衝突してしまいました。1928 年、各人はそれぞれの装置の特許を取得したのをご存じでしたか?
以上、私が1952 年にカリフォルニアに行ったときの状況を、経過を踏まえかいつまんで述べました。当時は、顎外牽引装置はまだ日常的に使われてはいませんでした。多くの人々はツイード氏の用例にしたがって治療を行う一方、顎外牽引装置を徐々に取り入れていきました。
 |
第5回 An Interview with Dr. Robert M. Ricketts 1987
2016.08.05
第5回 :A New Start 新天地カリフォルニア
Copyright © 2015 University of Michigan School of Dentistry
Some rights reserved. Except where otherwise noted, this work is licensed under the following:
Attribution: Please attribute the work to the University of Michigan School of Dentistry and any individual author(s) cited.
Not-for-profit: Use, display, and redistribute all or part of this work for non-profit and educational purposes only.
Share alike: Redistribute derivative works with the license listed here.
Visit the University of Michigan School of Dentistry’s website at
http://www.dent.umich.edu/.
View the original interview at https://www.youtube.com/watch?
v=lcBLmVOn3m0.
Interview conducted by James McNamara, DDS, MS, PhD.
Interview transcribed by Yuri Shindo, MD.
Interview translated by Katsuyuki Shindo, DDS, PhD.
【 A New Start 】
〔M.〕 Why did you leave Illinois? What was the reason why you went to California?
【 新天地カリフォルニアへ 】
〔M.〕 イリノイ大学を離れてカリフォルニアに行った理由をお聞かせ下さい。
〔R.〕 First, I was still under Brodie’s thumb. Even when I would publish, he would go over my papers and there would always be a little bit of Brodie in my work. I felt that I didn’t have the freedom that I wanted. As long as I stayed in an institution, I felt that I was still obligated to cooperate with the status of the whole thing.
Second, I married a woman from California and had relatives in California. I felt that there were opportunities there that I wouldn’t have where I was. I knew that Cecil Steiner, Hayes Nance, and Charles Tweed were in the Edward Angle Southern California Orthodontic Society. I knew that there was a great deal of progressive thought that was going on out there and I wanted to be a part of it. I also felt that I would have more freedom to do things out there than in the Midwest. So that combination of factors took me to California.
Brodie did his best to try to talk me out of it. In fact, in a letter he wrote“, I think California is a good place for you to go if your brain is dead.”I found out that there are more PhDs per capita in California than in any other state. After I started my practice and research, I was still asked to go speak. I got on the circuit starting in 1950. I got up to explain my research findings, the innovative things that we were doing, and where we thought things were leading. It wasn’t long before I began to have visitors. Entire study clubs would come and be with me in my practice for a day. So I recognized that people wanted to learn, and people needed to learn.
Now, who do you think was responsible for the formation of extra courses? You’re sitting down, right? Bob Moyers. He visited me in California and said“, Rick, we’ve got to get you back because some of the things you’re doing are just marvelous.”You know how exciting Bob is, and he just thought it was wonderful. I have to give Bob a lot of credit because he was one of the very few people who encouraged me. You have to understand that at that time, I was receiving criticism all of the time. Everywhere I went, I would be in fights. I’ve walked down the hall after giving a lecture, and everybody would turn their backs to me so they wouldn’t have to look me in the eye. They wouldn’t say that it was good or bad, or that they were indifferent. But Bob encouraged me.
〔R.〕 やはりブローディ教授の指示に従わねばならぬことには変わりがなく、独自の研究論文を出すにも彼の筆は必ず入りました。そのため、とにかく自由に活動できる場を欲しいと常日頃考えていました。研究室に在籍している限り、周囲に歩調を合わせなくてはならず、これにも煩わしさを覚えました。二番目の理由はカリフォルニアの女性と結婚したことです。同州には親戚もいました。カリフォルニアなら大きな可能性が拓けるとも感じられました。というのも、南カリフォルニアのアングル学会に所属していたセシル・シュタイナー、ヘイズ・ナンス、チャールズ・ツイードらがs活動を展開していたからです。そこは革新に溢れ、自分を試すには 最適な場所と思われたのです。少なくとも中西部に留まるより自由な活動が保証されるに違いないと確信していました。ともあれ、複数の理由が重なり、カリフォルニア行きを決断した次第です。
「脳みそがイカレてしまったらカリフォルニアほど楽しい場所はないだろうね」と、私がカリフォルニア行きを思い留るように一風変わった賛辞をブローディ教授は手紙にしたためてくれましたが...(笑)。PhDの取得者が (歯科医師数からみた比率では全国でもっとも多い同州において診療と研究活動をはじめた後も、講演の依頼が絶えまなく舞い込んできました。研究から得た知見、臨床で実地採用をしている考案の数々、時代の先端を行く思想を、1950 年以来説いてまわっていたからです。まもなく臨床見学者やスタディーグループの来訪が増え、彼らと診療所で1 日を過ごすことが多くなりました。私にははっきりと感触されました... 人々は学ぶことに熱心であり、またその必要があると。
特別コースの開設にあたり、責任者はどなただったかご存じですか?あなたはその人のすぐ近くに座っていましたよ...ボブ・モイヤーです。
彼は 1963 年にカリフォルニアまでわざわざ足を運んでくれて「リック、戻ってきてくれないものかな? 君の臨床と研究にはまったく目を見張ってしまうよ!」と興奮気味に話していました。私の仕事を高く評価してくれていたのです。私自身、当時からボブには深い信頼を寄せていました。私を勇気づけてくれた数少ない方のひとりだったからです。当時の情勢やら風潮を顧みて頂ければお分かりの通り、常に私は批判の矢面に立たされていました。どこに出かけようが論争が絶えず、講義が終わって講堂を歩き去るとき、人々は私の視線を避けるために背を向ける有り様だったのです。善し悪しの論議ではなく、ただ冷淡な仕草をもって私に対峙したのです。でもボブは違いました。
〔M.〕 When was this? What years are you talking about?
〔M.〕 いつの出来事? 何年ですか?
〔R.〕 We’re talking about 1962 or 1963. Bob came back and started talking about the things that I was doing and he said“, We’ve got to get your stuff in the University of Michigan. I’ve got a man back there who’s just the guy that I want to get your work.
His name is Bob Aldrich.”So I came at Bob’s invitation and put on a two-and-a-half day course for the alumni at the University of Michigan. After the third day, I went to Bob Aldrich’s home and he said“, We like what you have, but we know that we can’t get it with you just passing through here. We want to come out, we want to pay you, and we want you to give us an organized course.
Please, will you do it?” It wasn’t the first invitation I’d received, and I said, “No, I’m not sure I want to get into this. I’m still doing research, and I’m not sure that I want to take this amount of time.” Ransom Westover, Bill Clause [needed for check], and Bill Clause, and Bill Heisel] were also there that night. Finally, after an hour of him talking to me, I agreed to put on a course for them. I then made some phone calls to other people who had wanted to take a course. In February of 1964, I put on the first post-graduate advanced orthodontics seminar, and that’s how it started.
〔R.〕 1962、3 年のことです。ボブは再び来訪し、いろいろと意見を交わしました。「ミシガン大学であなたの助手にふさわしい人材を見つけましたよ。あなたのコースを手伝うにはうってつけの人物だと思う。名前はボブ・オードリッヒ。」と私に伝えました。そこでボブ・モイヤーの招待を受けてミシガン大学で医局卒業生を対象にした二日半のコースを開きました。三日目にボブ・オードリッヒ氏の自宅に案内され、彼から「あなたの思想に感銘を受けましたが、ここだけではとてもとても吸収しきれません。あなたの診療所に我々の方から出向いて是非ともご教授を願いたい。もちろん支払いの用意がありますので、組織立てしたコースを開催して頂けませんか?」との申し出がありました。この種の依頼ははじめてではありませんでしたが、とにかく「その時期かどうかは分かりませんし、まだまだ中途の研究やら片付けるべき仕事がたまっています。講習会の準備や開催に時間を割いてよいのかも判断がつきかねます。」と返答しました。ランソム・ウェストーバー氏、ビル・クラウス氏、ビル・ハイゼル氏らがその晩に同席していました。1 時間ほど話を交わして、とうとう彼らを対象にしたポストグラジュエートコースの開催を承諾しました。そこで、受講を希望しそうな知人らにも電話で誘いをかけてみることにしました。
1964 年 2 月、こうして卒後ポストグラジュエートのセミナーがはじまったのです。
 |
第4回 An Interview with Dr. Robert M. Ricketts 1987
2016.07.06
第4回:Influential Teachers 人を動かす三つの鍵
Copyright © 2015 University of Michigan School of Dentistry
Some rights reserved. Except where otherwise noted, this work is licensed under the following:
Attribution: Please attribute the work to the University of Michigan School of Dentistry and any individual author(s) cited. Not-for-profit: Use, display, and redistribute all or part of this work for non-profit and educational purposes only.
Share alike: Redistribute derivative works with the license listed here.
Visit the University of Michigan School of Dentistry’s website at http://www.dent.umich.edu/.View the original interview at https://www.youtube.com/watch?v=lcBLmVOn3m0.
Interview conducted by James McNamara, DDS, MS, PhD. Interview transcribed by Yuri Shindo, MD.Interview translated by Katsuyuki Shindo, DDS, PhD.
【 The Human Drive 】
〔M.〕 You told me the other day that you’re probably working harder now than you have at any time in your life. So you’ve had a very long history of being an over-achiever in a good sense. What drives you? What makes you go? What is it that made you do all of the things you’ve done in your career?
【 人を動かす三つの鍵 】
〔M.〕 先日の話では、今がいちばん精力的に仕事に励んでいらっしゃるとのことですが、生来的な良識にさらに磨きをかける努力を、長年にわたって持続し続ける原動力について、是非お聞かせ下さい。
〔R.〕 Well, I keep referring back to the work of Robert Ardrey. There are three things that motivate people, that give them their drive. The first is Identity. To understand Identity, you have to understand its antithesis, which is Anonymity. In other words, I have to keep convincing myself that I’m somebody. Certainly, it’s not that I have a bad opinion of myself, but I still feel that I have a potential that I haven’t filled yet. That’s what keeps me going. I still feel that my job isn’t done. I still feel that there is more to learn and more of a contribution that Robert M. Ricketts has to make.The second most overwhelming drive that we have is Stimulation, and its antithesis is Boredom. I’m highly curious and find research stimulating. It’s interesting to me, and I want to learn more. The pursuit of knowledge is just about as much of a pursuit as anything you could ever ask for in a human life.
The third motivation that we have is Security, and its antithesis is Anxiety. That’s the lowest in the hierarchy. I don’t think that Security is something that I have been motivated by for a long time. So the first thing that keeps me going is the fact that I still feel that I haven’t accomplished all of my potential goals. The second thing is that god, I’m having fun! It’s just wonderful to travel around the world, and to have the respect of all of the people that I’ve met. I’ve developed real love and friendships through orthodontics, and owe it a great deal. I think it’s marvelous.
The two things that I believe I have are (1) I have a natural curiosity, and (2) I keep developing my intellectual background. I think these have prepared me to do the things that I’ve done, and have motivated me to continue.
〔R.〕 これについては、ロバート・オーデリーの著作に照らしてお話しするのが便宜でしょう。人を行動に駆り立てる「衝動(ヒューマンドライブ)」として、彼は三つ要素を抽出し、著書の中で示しました("The Territorial Imperative" 第九章 Three Face of Janus(1967)。
一番目は、「自分が誰かでありたい」との確信を保ち続けさせるヒューマンドライブです。アイデンティティの対義語はアナニミティ(無名、 没個性)。その確信を得ようと私ももがき続けてきました。確かに、自分自身に対して否定的見解を抱いてはいなかったものの、未だ充足されていない潜在力を常に感じ、これに応えようと己を奮い立たせ前進し続けてきたと思います。現状満足に堕することなく、成すべき仕事はまだまだあり、過去のリケッツが乗り越えてきた仕事より、さらに多くを学び人々に貢献すべく、今も自分を鼓舞し続けています。
二番目の強力なヒューマンドライブは、「刺激(高揚)」です。刺激の反対はうんざりするほどの退屈感。好奇心が旺盛だからこそ探究心が高まり、探究心に促されて人は倦むところを知りません。振り返れば、研究そのものが私を刺激し、もっと多くを学びたいと欲する原動力になってい たことには興味がもたれます。人間が生きてゆく上で要請されるのは、た ぶん物事の真相を分かりたいという純粋な好奇心でしょう。
そして三番目のヒューマンドライブは、食糧・居住・治安・体の健康といった「安全性の確保(身の保全)」です。対義語は「不安」となりましょう。オーデリーによれば、安全性の確保はこれらの階層の中で一番下に配置されます。社会上の身の保全は暮らしの基盤となるので勿論大事なのですが、どうも私は長年このドライブだけに動かされて生きてきたようには思われません。まだ自分が十分責務を果たし得たようには感じられないことからも、一番目の要素こそが私を潜在的な目標に向かって衝き動 かしていた本体のようです。我ながら照れてしまいますが、二番目の要素はまさしく私の生き様そのものですね。世界中を訪ね歩いて出会う人々を 尊重し、交誼と友情を培う...、これは矯正歯科を通してこそ、はじめて味 わい得ることといえましょう。素晴らしいことです。
生来の資質の中で、私が摺れ枯らすことなく抱き続けているのは、 一つは好奇心、もう一つは知的背景を絶えず高める指向性zす。これらは 今までの業績や持続の原動力となっています。
〔M.〕 Now, we’re sitting here today in a very formal university setting. When you left Illinois, did you expect that you would end up working in a private institution of your own creation rather than a public institution? Was that part of the plan, or was that just the direction your life went after Illinois?
〔M.〕 大学内の公式の場におけるインタビューとはいえお聞きしたいのですが、イリノイ大学を去ることになったのは、大学機関よりもご自身の研究機関で独創的な能力を発揮させるご意向だったのでしょうか? そのような計画をお持ちだったのでしょうか、あるいはイリノイ大学を去ったあとの自然の流れでそうなったのでしょうか?
〔R.〕 No, it wasn’t planned at all. By the time I left Illinois, I had developed techniques in laminography. These techniques could give us a better understanding of orthodontics and growth by visualizing the joint. Later, I worked out a technique of projecting growth and treatment changes simultaneously by drawing up a patient’s plan on paper. This allowed us to work out the anchorages necessary to achieve and monitor our treatment goals. All of that had been worked out.
In addition, I had experiences with lathes as a farm boy. When I was twelve years old, I was so small that I could crawl into a threshing machine and fix it for my dad. I’d pick up a piece of wood and carve a tooth on it. I always had imagination and mechanical ability. So even before I left Illinois, I was making innovations. In fact, Brodie came to me one time and told me that I was no longer wanted to supervise cases in the clinic. The reason for it was that I was changing technique. He said,
“Why don’t you just take all of the crud that we have and finish it up for us? If you do, then you can give a course to the graduate students on occlusion and TMJ from its total aspect.”I said“, That’s fine with me because I want to be free to do the things I want to do anyway”.
〔R.〕 そのような計画は毛頭ありませんでした。イリノイ大学を退職するまでに技術開発を終えたラミナグラフィーは、顎関節を視覚化出来る点に優れており、臨床で実際に起こっている変化と成長発育の様相をこれによって知ることができました。引き続き、顔と歯列の成長を予測する技術と、治療による変化を客観的に評価する重ね合わせ法の双方につきましては、側貌セファログラムのトレース図から治療計画を紙の上で立案する技術の開発途上に確立しました。これに伴い、(歯列を動かすときに) 必要とされる大臼歯のアンカレッジをあらかじめ見積もることができるようになったばかりか、目標に向かって治療が順当に進んでいるのか否かをモニターリングすることも可能になりました。これらはみな同時期に実現したものです。
ところで私は、農場育ちの少年として旋盤を使いこなすといった下地は積んで来ました。12 歳の時は体が小ぶりだったので、故障した脱穀機の中に入って欠けた歯車の歯を木切れから削り出して父のために修理をしたり、とにかく想像をふくらませるのが好きで、生活の中では機械に慣れ親しんでいました。そのため、イリノイ大学を去る以前から、様々な考案やら発明が拓けてきたわけでしょう。あるときブローディ教授から、「きっと、もうこれ以上は、治療を監督してもらわないよう望んでいるんだろうね。」と言われました。というのも私が次々に治療手技を刷新していったので、ブローディ教授としても当惑していらしたのでしょう。さらに彼から、「山積みになったその資料を片っ端からかたづけてくれるかね? もし引き受けてくれるというなら、基礎関連のあらゆる分野を統括した咬合と TMJ の大学院生向け講座を君に担当させてもよかろう。」と伝えられたので、「私なりの方法で自由に臨床や研究を行うことを希望しておりますので、喜んでお引き受け致します」と返答しました。
 |
第3回 An Interview with Dr. Robert M. Ricketts 1987
2016.06.17
第3回:Postgraduate Work イリノイ大学へ
Copyright © 2015 University of Michigan School of Dentistry
Some rights reserved. Except where otherwise noted, this work is licensed under the following:
Attribution: Please attribute the work to the University of Michigan School of Dentistry and any individual author(s) cited. Not-for-profit: Use, display, and redistribute all or part of this work for non-profit and educational purposes only.
Share alike: Redistribute derivative works with the license listed here.
Visit the University of Michigan School of Dentistry’s website at http://www.dent.umich.edu/.View the original interview at https://www.youtube.com/watch?v=lcBLmVOn3m0.
Interview conducted by James McNamara, DDS, MS, PhD. Interview transcribed by Yuri Shindo, MD.Interview translated by Katsuyuki Shindo, DDS, PhD.
【 Influential Teachers 】
〔M.〕 What kind of a teacher was Brodie? In other words, what kind of interactions did he have with his students?
【 受け継がれる指導力 】
〔M.〕ブローディ教授の指導の特徴とは? また生徒との間にどのような展開が生まれる教え方だったのですか?
〔R.〕 I’ve often said that there are four or five ways of teaching, and that the true seminar way of being a leader of a discussion is probably the number one most effective way of teaching. You teach by asking questions. An intelligent person who knows his subject knows which questions to ask that will lead to the next one and so forth to ultimately get the message across into the student’s mind.
The nice thing about teaching in this manner is that the thought that comes belongs to the student. It’s nothing that is forced on him, rather it’s something that was already an established pathway in his brain. So it is a method of not only teaching, but also of information retention. This becomes highly stimulating.
The other part about it was that it wasn’t just bands and teeth. It was biology. It was geography. It was geology. It was the issues of the day. It was politics. It was religion. It was just about any subject that came along, so it wasn’t just about learning to be a clinical orthodontist. I always said it was about learning to be a man or a woman. An adult thinker. And this was what Brodie was about and this was the grasp that he had on the students that really was prevailing.
〔R.〕 日頃話していることですが、教育方法は 4、5 種類に分類されます。ディスカッション式にリーダーが先導してゆくセミナーは、その中でも教育の真髄を発揮させるのに最大の効があります。適切な問いを投げかけ、それによって教育啓蒙をはかるやり方です。主題に熟知している者が生徒に対して意見を求め、さらにその答えが周囲を刺激するかたちで次々に回していく... そうして生徒の心にメッセージを刻んでゆく方法です。
この方法の優れた点は、思考過程そのものが身についていく点です。強いるのではなく、おのずと考える筋道を補強していきます。生徒はこうして情報の全貌を把握しますが、それに付随して記憶を活性化させることも出来ます。しかもこのとき受けた刺激は長く心にとどまり、人を高揚させてくれます。
ブローディ教授の話題は歯やバンドに限局したものではありませんでした。生物学、地理学、地質学、日々の話題や社会的な出来事、政治、宗教等々の全般にわたりました。単に専門医を育てることにとどまらず、社会常識をわきまえた上で成熟した思考を駆使できる一個の人間になれ、と鼓舞されたものです。ブローディ教授の関心もここに注がれ、生徒を把握する器の大きさがそこには感じられました。
〔M.〕 Do you think that there’s anybody in orthodontics today that would fall in the same mold or have the same stature that Brodie had when you were a student?
〔M.〕 今日の矯正歯科界で、ブローディ教授のような傑出した教育法やその才覚を備えもつ人物をご存じですか?
〔R.〕 I don’t think so. I think we’re dealing with a brand of society that unfortunately is waiting to be entertained rather than entertaining themselves. That is waiting to be educated rather than educating themselves. That has somehow lost the joy of the pursuit. I don’t know exactly all of the social factors that are involved, but it’s going to be a rare student that comes along now that’s going to catch this flame. They’re bound to be there, but I don’t know who it would be right now. I think that even if an educator like Brodie came along today, our social problems are such that he wouldn’t dare treat students in the manner that Brodie treated them to make the most out of them. I discussed this with Brodie many times, but he had the idea that the very moment you tell a student that what he does is acceptable, the student is going to become complacent and fail to grow. If he thinks he’s already there, why should he work any harder? So any time you give too many compliments, you are killing the incentive, at least at that level of education. Maybe it’s appropriate if you have a child that needs some encouragement, patting on the back, loving, and so forth. But by the time students reach an age when they should have maturity, I don’t think that compliments are going to ultimately get the most out of a student in his career. I really don’t believe so. That’s what Brodie had.
He got that from Angle, because that was also Angle’s philosophy in teaching. Look at the impact that Angle and Brodie had, particularly in education.
〔R.〕どうも見当たりません。不幸にも今日の情勢は、「自らを楽しむ能動性が失われ、誰かがもてなしてくれるのをぼんやりと待ち、自らの手で自分を教育する積極性が萎え、教えてもらう事をもって教育と錯誤する...」、そんな有り様です。本当は何だろう?... 旺盛な好奇心に駆られて真実を追求する醍醐味が失われてしまった観があります。この色褪せた状況を招いた原因のすべてについて到底私に分かるはずなどありませんが、(アングル、ブローディ、リケッツ... と連綿と続いてきている生物学を基 盤に据えた)統合的臨床をしかと受けて立つ生徒は、もう稀になりました。 自らを束縛していることすら気づかぬ人が増えてしまいましたが、誰かはいるでしょう。しかし、仮にブローディ教授のような有能な教育者がいたとしても、彼と同様に生徒の才能を最大限に伸ばす扱い方は、周辺の事情を察してあえて差し控えるかもしれません。
このことに関して、ブローディ教授と私は幾度も意見を交わしました。その中で彼は、「教え子が伸びる機をとらえて褒めてやらないと伸びないが一方で、すでに分かり得ていると生徒が自惚れたら努力を惜しんでしまい、かえってその芽を摘み取ってしまいかねない」、と話していました。 勿論これは初期教育の話ですが...。例えば、我が子を育てる過程では、勇気づけたり優しくなだめるのが有効な場面もありますが、ある年齢に達する前に独立心を養っておかねばなりません。それゆえに、時宜に適う「褒め」 かたをすることは大切とはいえ、それだけでは教育の体を成さない事も、 充分に指導者は踏まえておくべきです。ブローディ教授はそのツボをわきまえていました。
これは「教育」という面において、彼がアングルから受け継いだ特筆すべき能力です。人材の育成に関して、アングルとブローディ教授の影 響力は絶大でした。親玉としてのブローディ教授の存在は際立っていまし た。
〔M.〕 Who else on the Illinois staff had an impact on your career?
〔M.〕 あなたの経歴にインパクトを与えたイリノイ大学のスタッフ は、ほかにいましたか?
〔R.〕 Well, of course Brodie was number one because he was the kingpin and he was the force.
He had taken the Charles Tweed course and was endowed with clinical capability and knowledge. He was in cephalometrics at that time, and don’t forget we got his analysis before it was even published. In fact, he was still working on it and was adding the last part of it, the lower incisor to the occlusal plane, at that time. So Downs was highly influential.
He’d come in on Fridays and our class would all meet for breakfast. We had a very close class and we used to have parties that would match any party you’ve ever heard of, because we were all intense and when we’d relax we would really have some great parties. It was all in fun, and our class is still very close. The people in it are still very close. It’s a genuine love that we have for each other. So Downs was like a father too.
〔R.〕 勿論ダウンズ先生も臨床実地に長けている点では同じでした。ツイードコースの訓練も受けたダウンズ先生は、臨床の力量と経験に秀でていて、当時はセファログラムの研究に従事し、かの有名なダウンズ分析法の発表前に我々はそれを臨床に応用していました。実際、彼はそ の分析法の最終部分に当たる、咬合平面に対する下顎前歯の位置づけについて研究をまとめ上げている最中でした。彼から受けた影響も大きいものでした。
毎週金曜日に医局を訪れるダウンズ先生を囲んで、我々医局生は朝食がてらミーティングを重ねました。クラスの仲間はとても親密で、折を見ては素晴らしいパーティを催したものです。というのも、矯正歯科という共通の目標に向かって互いの気持ちが一体化しており、時には大いにくつろぐ事が出来たからです。医局生相互の深い交誼は今も変わりません。 純情の輪とは、まさしくこのことでしょう。それもこれもダウンズ先生のお陰ですから、父親のような存在でした。
〔M.〕 Who else?
〔M.〕 ほかに誰か?
〔R.〕 Earl Renfroe was a junior member on the staff, and he assisted Brodie. Al Moore was there for a few months in the beginning before he went to Washington. We still saw the influence of Abraham Goldstein and Ernes Meyer. Jerry Baucher and Bill Blewer were junior members of the staff who stayed on and helped a little bit. Essentially, that was the staff. We also had many lectures from Maury Massler. We were met with open arms when we’d go down to Isaac Schour’s department in histology. I had a wonderful rapport with the people in anatomy and physiology. I was the person who got Pruzansky interested in his original work in electromyography with the Department of Physical Therapy in the medical school. Andrew Ivy was doing a lot of his research at that time so there were many medical students that we could converse with. We would meet with them in the YMCA, Greek Restaurant, and so forth around the university at that time. So that was the atmosphere.
〔R.〕ブローディ教授を補佐したアール・レンフロー、ワシントンに赴任する前に数ヶ月ご一緒させていただいたアル・モアー、そのほかアブラハム・ゴールドシュタイン、アーネス・メイヤー、ジェリー・バウシャー、ビル・ブロウアーといった若い指導医局員らの影響もありましたが、あくまでも医局のスタッフでした。下の階にあったアイザック・シャワー教授の組織学教室に集った我々へ(イリノイ大学で小児歯科教室を創設した) マリー・メズラー先生はしばしば講義を施してくれました。解剖学と生理学の仲間とも親しく接していました。医学部の理学療法科で筋電計を用いた研究に打ち込んでいたプルザンスキー氏と懇意になれたのもこの頃です。アンドルー・アイヴィー氏も多くの研究(※ 咽頭部の成長研究等)を 推し進めていた時期で、医学部生と大学周辺の YMCA やギリシャ料理のレストランなどで意見を交わす、そのような恵まれた雰囲気でした。
〔M.〕 If you could step back, and you could look at Bob Ricketts circa 1947, what would you describe? What were you like?
〔M.〕 顧みて、その頃のご自身をどんな人間だったと思いますか?
〔R.〕 I was a fun-loving person. I had played football, and had been a dance instructor. I wouldn’t say that I was a lady’s man, but I wouldn’t run the other way. I think I was hungry. I’d come from a farm, and I think I wanted to make something of myself. I’d taken a year off from school to work in steel mills and a radio factory - Delco Electronics which made General Motor radios - and had gotten a little introduction to electronics. I worked with metals in the wire and steel mills. I was hungry. Underneath, I also had a tremendous ethic. I wanted to do something for people, and I was highly curious and imaginative. I think I came prepared because for the two years that I was in the navy, I studied something and read the literature almost every day. When I went to Illinois, I was versed in anatomy from three t e x t b o o k s . I f s o m e b o d y a s k e d m e a b o u t a p a r t i c u l a r t h i n g , I ’d s a y “, W e l l which book do you want it from?”, because they wouldn’t all be the same. So that’s the kind of student I was when I got there.
〔R.〕 フットボールに打ち込み、ダンス教師で楽しみながら稼ぐ... とにかく刺激的な対象に向って楽しみを謳歌する性格でした。女ったらしではありませんでしたが、女性には惹かれる向きは無きにしもあらず... といったところでしょうか。貧乏学生の例外にもれず、日々の糧には飢えていたと思います。とにかく農家の出なので自立心は旺盛でした。学費を稼がねばならなかったので一年の休学中に製鉄所や電気機器工場(ジェネラルモーターズにカーラジオを納めていたデリコエレクトリ社)へ勤め、電子工学の基礎は少々身につけ、また金属線の加工や製鉄技術も経験しまし た。とにかく働かないと学費の工面ができない時期でした。また一方で、 驚くほど倫理的に自己規制を課す趣が私の底面には流れており、人のために尽くしたいと願う一方、好奇心に任せて旺盛に想像力をふくらませていました。海軍に2年間勤務していたとき、日々さまざまな学術書や文芸書を読み漁り、イリノイ大学に入局したときには 3 冊の解剖学書を熟知していたので、なにか訊かれると、「どの本の意見を聞きたいのですか?」と答えるぐらいでした。なにせ、各々の本の内容が違っていたからです。そんな生徒でした。
 |
第2回 An Interview with Dr. Robert M. Ricketts 1987
2016.06.11
第2回:Postgraduate Work イリノイ大学へ
Copyright © 2015 University of Michigan School of Dentistry
Some rights reserved. Except where otherwise noted, this work is licensed under the following:
Attribution: Please attribute the work to the University of Michigan School of Dentistry and any individual author(s) cited. Not-for-profit: Use, display, and redistribute all or part of this work for non-profit and educational purposes only.
Interview conducted by James McNamara, DDS, MS, PhD.
Interview transcribed by Yuri Shindo, MD.
Interview translated by Katsuyuki Shindo, DDS, PhD.
【 Postgraduate Work 】
〔M.〕 Now how much cephalometrics was used in the program when you entered?
【 イリノイ大学へ 】
〔M.〕 入局のころ、卒後教育でどれ程セファロは活用されていましたか?
〔R.〕 In 1947, William B. Downs was still collecting his material, which he published in 1948. We did receive the Downs analysis. The class ahead of me, however, used their cephalometrics analysis from physiologic rest position. Of course, by that time Downs had given that up. Originally, it had been done at Brodie’s insistence, I think, because the prevailing thought at that time was that everything emanated from rest position, that was a constant thing, and that’s what you had to treat. Part of my original work discharged that idea altogether.
〔R.〕 頭蓋計測機器として使われていたセファログラムをはじめて臨床に導入したのは、ダウンズ先生です。1947年、彼は目下翌年発表されることになる研究資料を集めている最中であり、Downs 分析法を我々は 学んでいました。生理的安静位を基準に計測を試みていた時代ですが、もちろん彼はこの考えを支持することをすでに控えていました。当初は、ブローディ教授の主張に沿って生理的安静位が採用されていたのです。つまり、ここがすべての起点であると信じられ、しかもそれは恒常性が保たれ、治療もそこに向かって進めればよい... そんな誤認が蔓延していました。後年、私の研究によってその考えは解消されましたが...。
〔M.〕 One of the things that I have seen in the last few years among our own residents here at Michigan is that they don’t really appreciate Brodie and what he did and where he fit into the whole scheme of orthodontics and orthodontic history. Can you give us a couple minutes on Brodie?
〔M.〕 ミシガン大学の研修医の間では、ブローディ教授の評判は近頃芳しくありません。彼が唱えた学説についても、歴史的な業績についても同様です。彼についてなにかコメントを頂けませんか?
〔R.〕 I suppose it started when I first heard of Brodie from Dean Crawford. When he asked me if I was going to go ahead and pursue this, he said“, Well there’s only one place to go and that is to Brodie in Illinois.” I said“, Why him?” He replied“, He’s the only one who’s going to teach you anything.” I thought that was rather strange considering how many dental schools were in the country. Naturally, I was interested in an interview with Brodie so, as I mentioned previously, I hitchhiked to Chicago. The minute that you walk in in the presence of Brodie, you get the idea that he is a very sophisticated and knowledgeable person, and one who has the ability to stimulate you. During that first interview, one of the students came in with a patient who had just been retained. I looked in the kid’s mouth and it was just beautiful. Brodie said“, Wouldn’t you like to do orthodontics this way? Wouldn’t you like to be able to do this?” I said“, Boy, would I !”This was just a part of Brodie.
Brodie was selected by Edward H. Angle, of all of the students that Angle had, to continue his flame. Before I left Illinois - I stayed there for five years - Brodie invited me to his home one night. It was just us and his wife, Vera. He said, “Did I ever read you my letters?” I said“, No, I think I’ve heard you talk about them but I’ve never read them.” He then reached up toward the top shelf of his library and pulled down a box labeled “letters”. With tears in his eyes, he read the handwritten letter from Angle notifying him that he had been chosen to carry on his work. Did you know this? Angle said that of all the students he’d had, Brodie had the talent. He hoped Brodie could carry on the goals that he had had during his career. I wondered why Brodie had done that to me. Maybe in Brodie’s own way, he was trying to tell me that I was the next in line to carry on this flame.
〔R.〕 クロフォード学長から、初めてブローディ教授の話を伺った折り、「すべてを教えられるのは、全米でもイリノイ大学のブローディ教授ひとりしかいない、その道を志すのであれば彼の許で学びなさい。」と伝えられ、数ある(※ 1945年当時は、全で 5 箇所の矯正歯科大学院コースがあった)歯科大学でなぜ一人なのか? と当初訝しく思いました。ともあれシカゴに出かけ彼に面会を求めることにしました。あふれんばかりの知性と人の気持ちを高揚してくれる才覚を彼が秘めていることは、一瞬であなたも観取されるに違いありません。実際、そのような人物だったのです。 面会のとき、一人の大学院生が保定処置に移行したばかりの患者を伴い入室してきました。患者の歯列に目をやるとその美しさに私はすっかり魅了され、そこへすかさずブローディ教授は「君もこのような矯正歯科治療をやってみたくはないかね?」と尋ねて来たので、即座に「もちろんです!」と私は答えました。こんなところにも彼の一面がうかがわれます。
アングルは多くの弟子の中からアングルの業績全容を受け継ぐに相応しい最高の後継者としてブローディ教授を選びました。5 年ほど過ごしたイリノイを私が去るある晩、ブローディ教授の自宅に招かれ、べラ夫人の同席する中、私は「あの手紙を君は読んだかね?」と訊かれ、「いいえ、話には伺ったことはありますが…でもまだ拝見したこともありません。」と 答えたところ、書棚の上の『手紙』と記された箱をおもむろに彼は降ろし、 アングル直筆の書簡を取り出すと、目に涙を潤わせながら「君にこそ託す…」 と読み上げてくれました。アングルは、アングル自身が成し遂げた業績を是非ともブローディ教授に受け継いでもらい、さらに生涯を賭して矯正歯科の発展という目標に邁進するよう希望を託していたのです。
いったい何を、そのような場を設けてまでしてブローディ教授は私に伝えたかったのでしょう? おそらくは、矯正歯科の骨子全体を私に継承 してもらいたいとの、彼なりの表現だったと思われる次第です。
〔M.〕 Do you think you’ve done that?
〔M.〕 その期待に応え得たとお考えですか?
〔R.〕 Yes. If I could be candid and objective, I think that I, more than anybody since Brodie, have tried to carry the whole feeling of biology and mechanics and tie the two of them together. I think that’s been one of my fortes. Brodie had this particular talent of stimulation. He made you feel that orthodontics was just about the most important thing you could do in your life. The students would get so excited that sleep was forgotten. It was so motivating to listen to him and being in that atmosphere was just so lifting; a whole transition among the students took place. When I went to Illinois in 1947, I weighed 196 pounds. When I went home that following Christmas, I weighed 164 pounds.
So I’d lost 32 pounds in about 4 months. My father saw me and said“, Good god, what are you trying to do ... kill yourself?” So that was the kind of conditioning that was there.
That was the kind of intensity that was there.
〔R.〕 率直に振り返り、なおかつ客観的に申し上げればそうなるでしょう。生物学、そして臨床メカニクス、それら両者の融合につとめたブローディ教授の試みに照らせば、そう申して差し支えはありません。私自身の業績の根幹も、そこに絞られているからです。ところで、人生の中で矯正歯科臨床こそが最も大事と思わせるほど、ブローディ教授は生徒を鼓舞させる才の持ち主であり、我々は彼の話に聞き入り寝食を忘れるほどの情熱的雰囲気に包まれていました。1947年にイリノイ大学に入局したとき、196 ポンド (90 キロ弱)あった私の体重は、クリスマスの帰省時に 164 ポンド (70 キロ半ば)まで激減、たった 4ヶ月でそんなに痩せてしまったものですから父親から「すこしは身のことも考えろ」と呆れられました。医局全体がほどばしる活気に満ちていました。
 |
第1回 An Interview with Dr. Robert M. Ricketts 1987
2016.06.07
第1回:Dental School 歯学部時代
Copyright © 2015 University of Michigan School of Dentistry
Some rights reserved. Except where otherwise noted, this work is licensed under the following:
Attribution: Please attribute the work to the University of Michigan School of Dentistry and any individual author(s) cited. Not-for-profit: Use, display, and redistribute all or part of this work for non-profit and educational purposes only.
Share alike: Redistribute derivative works with the license listed here.
Visit the University of Michigan School of Dentistry’s website at
http://www.dent.umich.edu/.View the original interview at
https://www.youtube.com/watch?v=lcBLmVOn3m0.
Interview conducted by James McNamara, DDS, MS, PhD.
Interview transcribed by Yuri Shindo, MD.
Interview translated by Katsuyuki Shindo, DDS, PhD.
【 Dental School 】
〔M.〕 Today I think we’ll start off by having Bob tell us a little bit about his own background and how he got involved in orthodontics. As we go along, we’ll get into more substantive issues with regard to orthodontic treatment in the past, the present, and hopefully the future.
【 歯学部時代 】
〔M.〕 今回は、リケッツ先生をお招きして、ご自身の背景と矯正歯科に携わるようになった経緯、さらには矯正歯科臨床の過去、現在、願わくば未来についてもお話を伺います。
〔R.〕 Well first of all, Jim, I’d like to thank you for the opportunity of being interviewed. As we said, I’m at an age in which I still have my faculties. I suppose the best way to describe my interest in orthodontics is by going back to my sophomore year in dental school. The first lecture that I heard in orthodontics was by Thomas Speidel. He was head of the department at that time at Indiana University, and I felt that orthodontics was the ultimate challenge in dentistry. So as a sophomore, I had an interview with the dean who was Bill Crawford at Indiana University and I told him that I was interested in orthodontics, and was probably going to be interested in graduate work and in research. All at once, he almost came out of his chair and said how glad he was because he’d helped me through my career from football into dentistry, which was a very difficult task. We learned at that time that we had courses in labio-lingual, so the first technique that I learned was the labio-lingual technique. Then in my senior year, I had the opportunity to actually start practicing orthodontics in dental school.
〔R.〕 お招きいただきありがとうございます、ジム。こう見えても 浩然の気を養っているつもりです(笑)。矯正歯科に興味を抱いたのは歯学部二年生に遡ります。インディアナ大学歯学部長トーマス・シュピーデル先生から矯正歯科学の講義を聴き、歯科では究極のチャレンジ分野であると直感しました。そこで早速二年生の時に、ビル・クロフォード学生部長に面会し卒後は矯正歯科の大学院に進んで臨床と研究に邁進したい旨を伝えたところ、まさに椅子から飛び上がらんばかりに彼は喜んでくれました。フットボール選手だった私が歯学部に入学するという難しい道のりを彼は陰で援助してくれた恩人でした。ラビオリンガル法を二年生当時は学んでいたのですが、上級生になると歯学部内で本格的な矯正歯科治療に触れる機会に恵まれました。
〔M.〕 Was that through the Department of Orthodontics?
〔M.〕 矯正歯科の診療科で学んだのですか?
〔R.〕 Yes, and the reason for it was that Speidel had left. He had taken over deanship at Loyola University in New Orleans and there was nobody to treat the cases that he had left behind. So this was left to the head of the Pedodontics Department, Drexall Boyd. And I bothered Boyd until he finally let me start putting in ideal arches, tying wires, and using ligatures and ligature-tying pliers. So in fact, I got interested in the edge-wise mechanism as a senior in dental school.
〔R.〕 シュピーデル歯学部長がニューオリンズのロヨラ大学の学生部長に招聘されると、彼の診ていた患者を引き継ぐ者がすぐには見つからなかったので、当面は小児歯科教室のドレクセル・ボイド教授に治療が委ねられました。そのとき、ボイド先生が渋々首を縦にふるまで私が騒ぎ立てたので、アイディアルアーチのセットから結紮、タイニングプライヤー の使い方を経験することが出来ました。つまりエッジワイズ治療に本格的に興味を抱いたのは、歯学部上級生のときです。
〔M.〕 And when did you go to dental school to begin with?
〔M.〕 歯科大学に進んだのはいつですか?
〔R.〕 I entered in in 1942, which was during the war, and I finished in 1945. Our program was a speed-up program so I went through dental school in two and two-thirds years.
〔R.〕 入学は1942年。戦時中でしたから歯学部教育は2年8ヶ月に短縮されました。
〔M.〕 Now did you go directly into orthodontics from there?
〔M.〕 そのまま矯正歯科教室へ進まれたのですか?
〔R.〕 In the very beginning of my junior year, I hitchhiked to Chicago and had an interview with Allan G. Brodie. I was admitted and was supposed to start orthodontics in September 1945. However, I had to go back to the military to serve two years as a navy dental officer. I was pretty bent out of shape at the time, but in retrospect I think it was a marvelous experience for me because it added to my knowledge base. By 1947, I think I was much better prepared than before, but by then there had been an accumulation of some people with good records. I was put as an alternate with - would you believe - Samuel Pruzansky and Robert McGongle. The three of us were the alternates who finally made it into the class. During my tour in the navy, I completely reviewed every textbook that I had in the four years of dental school and two years in the navy.
〔R.〕 ヒッチハイクでシカゴに出かけ、アーレン・ブローディ教授に面会を求めたのが三年生に上ってすぐの頃です。いよいよ(歯学部を卒業する)1945年の9月、矯正歯科を本格的に学ぶことができると思いきや、軍から招集され歯科軍医として海軍に入隊、予定通りにことは運びませんでした。しかし今振り返りますと、基礎知識を蓄積する素晴らしい経験に恵まれたと思います。優秀な人との交流も増えて1947年までには以前よりだいぶ私自身の準備が整ったように思われます。入局に当たって私は補欠組でしたが、そこに後年頭角を現すサシェル・プルザンスキー氏、ロバート・マッガンゴル氏もいたとはとても信じて頂けないでしょう。最終的には三人とも入局を許可されましたが、歯学部で学んだすべての本を海軍時代の2年間におさらいしました。
〔M.〕 Now part of your coursework, particularly the course that you offer in your own office facility, stresses anatomy very heavily. Where did that all come from?
〔M.〕 臨床能力を発揮するために、解剖学をしっかり抑えておくよ うにと、とくにご自身のコースでは強調なさるとともに、そのための資料や準備を充実させていらっしゃる理由をお聞かせ下さい。
〔R.〕 I’m not exactly sure. I always liked anatomy and physiology, and I always felt that if you didn’t know your anatomy, you were pretty much lost when it came to discussing any of the details of function and physiology. I always felt that anatomy was the basic reference, and that osteology was the foremost reference that anyone can have. If you didn’t have that, you didn’t have an orientation; if you didn’t have an orientation, you couldn’t learn.
〔R.〕 明確な理由があったと感じられませんが、解剖学と生理学には以前から惹かれるものがありました。でも解剖学を知らなければ機能学、生理学の詳細を知ることはできません。解剖学は基礎的な指標を把握する上で欠かさるべきものであり、就中、骨学は大切です。骨学を理解していなければ構造特性の指標は捉えるどころがなく、その指標がわからないと(機能を含めた構成体の全貌を)学びようがありません。
 |
「サイエンス」って?
2016.03.23
『We have a science in order to protect ourselves』
Bioprogressiveの、見えない真髄です(笑)。
Truth, Principle, Mind, Facts, Investigation, Research, Science, Art,Quality, Discipline, Learning をキーワードとしてアリゾナのRickettsセミナーでは語られていました。
● Truth(知りたいと欲するいわば目標:人間には動物の能力としてかなりの限界があり、しかも事実誤認を犯しやすい存在)
● Principle(一般には適用可能な原理原則、でも自然界の複雑事象とヴァリエーションに照らせば例外もあり。臨床ではおおいに活用したい!!)
● Mind(真実を求めるには「心」の助けも借りる。クールな論理と豊かな経験をベースに明察をふかめる)
● Facts(Mindを最大活用して事実を曇りなき眼で捉える。でもまずは「色眼鏡」を外す努力から!)
● Investigation(システマティックな研究と実験の構築)
● Research (仮説の検討やら検証に挑む! 心身を害する無理な意気込みは禁物・・・「待てば海路の日和あり!」ですね)
● Science(「4つの科学手法(※機会を見て解説)」を活用して実証、しばしば自身の仮説を否定・・・理論の積み上げは、ある種の破壊作業)
● Art(技=臨床では自力で実証。哲学や人文学の領域では生き様として実証。末節の臨床手技に慢心せずに「教養」の奥深さを知ること!)
● Quality(卓越した生産と稔り、ゆるぎない確信、そして落着)
● Discipline(人々との関わりで染みついた己が思考の修正。つまり生涯Progression! 余力あらば周囲も啓蒙、ともに楽しむ!)
● Learning (knowledge=知(チ) / understanding=得心 / responsibility=ようやく世間様に申し訳が立つ程度に、責任を持てる臨床人になる=論語なら差し詰め「成人」かな?)
この過程がふらつくと・・・Communication (意思疎通)からしてつまずきがち。が、善し悪しの問題ではなく、それも臨床人各自の特性。でも野生動物は決してミスしません。
最たる結果は・・・
What is said, what is meant and what is understood, maybe different!!
(What he says, what he means, what they understand, maybe different.)
グルリと一巡して、
『We have a science in order to protect ourselves』
以上が、Ricketts R. M. つまりBioprogressiveで提唱される「自然科学のいろは」。身の安全をはかり思考の地盤を固めるための援用とみてみましょう。
 |
 |
 |
うぐいすの みをさかさまに 初音かな(宝井其角)
2016.03.01
うぐいすの みをさかさまに 初音かな(宝井其角) 江戸市中評判の句。診療所ちかくの里山‥‥ひんやりした朝に響き渡る初音を耳に、一日の始まりです。
久々に、Provocations and Perceptions in Cranio-Facial Orthopedicsの冒頭文を意訳してみました。Dr. R. M. Rickettsの生き様がにじみ出ています。
20年前に読んだときと印象がちがっているのは、自分もかわってきたからでしょう。
 Provocations and Perceptions in Cranio-Facial Orthopedics 序文
Provocations and Perceptions in Cranio-Facial Orthopedics 序文
 |

